Download
1 / 11
160 likes | 520 Views
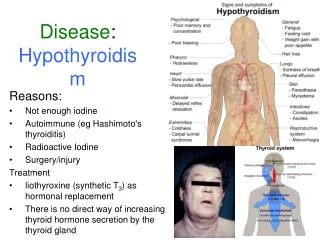
Disease : Hypothyroidism. Reasons: Not enough iodine Autoimmune ( eg Hashimoto's thyroiditis) Radioactive Iodine Surgery/injury Treatment liothyroxine (synthetic T 3 ) as hormonal replacement There is no direct way of increasing thyroid hormone secretion by the thyroid gland.

E N D
Disease: Hypothyroidism Reasons: Not enough iodine Autoimmune (eg Hashimoto's thyroiditis) Radioactive Iodine Surgery/injury Treatment liothyroxine(synthetic T3) as hormonal replacement There is no direct way of increasing thyroid hormone secretion by the thyroid gland
Targets: thyroid hormone carriers Sample Presentation Slide 2 • In human plasma, T3 & T4 are >99% bound to carrier proteins • Reference range in normal adult blood: • Free (only free hormone is active) • T3: 3-8 pmol/L • T4: 10-20 pmol/L • Total T3/T4: 1-2.5 nmol/L (~ 100-fold higher than free) • 70% bound to thyroxine-binding globulin, TBG • 10-15% to transthyretin, TTR (same as thyroxine-binding prealbumin, TBPA) • 15-20% to albumin TBG TTR Albumin
Sample Presentation Slide 3 Targets: Additional role of TH carriers in drug-drug interactions for other drugs • Because >99% of T3/T4 are protein-bound in plasma, carrier protein disregulation may lead to large variations in free T3/T4 • Factors that may change TBG concentration: • pregnancy, estrogen-containing medication (TBG) • infectious hepatitis (TBG) • nephrosis, acromegaly (TBG) • androgen or corticosteroid therapy (TBG) • T3/T4 binding by TTR is inhibited by salicylates. TBG TTR
Transactivation domain DNA binding domain Ligand-binding domain 1 53 127 190 410 THR1 THR2 THR1 THR2 1 53 127 190 370 490 1 107 181 244 461 1 122 196 259 476 Hormone or agonist therapeutic Cell Type II Nuclear Hormone Receptor (e.g. THR) Nucleus Unbound or antagonist-bound (inactive) Agonist-bound (initiates gene transcription) = Co-repressor Co-activator + RNA polymerase DNA HRE target gene HRE target gene Ligand-binding domain of THR1 in complex with T3, PDB 3gws Sample Presentation Slide 4 Target: Human Thyroid Hormone Receptor • Two main types ( and ), each having 2 isoforms • Length: 410-490 AA • MW ~ 46.8-54.8 kDa • Tissues: multiple • Cellular localization: nucleus
Drugs:Liothyronineand Levothyroxine Sample Presentation Slide 5 • Thyroid hormones (TH) and their synthetic analogs increase oxidative metabolism of carbohydrates, lipids and proteins by the mitochondria. • They also increase the number of catecholamine (e.g. adrenaline) receptors on target cells, thereby increasing catecholamine sensitivity – may aggravate heart conditions; acute overdose may lead to heart failure • Indications: hormone replacement therapy for hypothyroidism and myxedema
Liothyronine and Levothyroxine:ionization, dissolution, and phase partitioning Sample Presentation Slide 5a Graph from: MCD
Liothyronine and Levothyroxine: Target binding Constants and Energies Sample Presentation Slide 6 • https://www.ebi.ac.uk/chembldb/ • Sandler B, et al. Thyroxine-thyroid hormone receptor interactions. J Biol Chem. 2004; 279(53):55801-8
Liothyronine and THRMolecular basis of drug-target interaction Sample Presentation Slide 7 • Van der Waals interactions: • Perfect steric fit between the ligand and the pocket many VW contacts • Electrostatics: • The three Arg in the bottom of the pocket create a strong positive charge interacting with the negatively charged carboxyl group of the drug.
Sample Presentation Slide 8 Liothyronine and THRMolecular basis of drug-target interaction • Hydrogen bonds: • Three residues make HBs with the ligand: Arg-282, Asn-331, and His-435 near the pocket entrance. The ligand has no unsatisfied hydrogen bond donors/acceptors. • Other types of interactions are not observed: • Two aromatic residues in the pocket, none of them makes a Pi-interaction. • No metal ions • Non-covalent interaction
Sample Presentation Slide 9 Liothyronine: LogP, PSA and lipophilicity • The surface of Liothyronine molecule is mostly non-polar • LogP = 3.9 Liothyronineis lipophilic • Levothyroxine has an additional iodine atom: LogP = 4.7, more lipophilic • PSA is 98A2 , good permeability ( < 140). • Has 4 freely rotatable and 3 restricted bonds Non-polar atoms Polar atoms
Introduction and conclusion Interesting aspects of pharmacodynamics and pharmacokinetics resulting from the drug properties described above. Bioavailability? Protein binding? Half life? Drug interactions? Past and future of the drug(s). Market and competition. Stage? OR: Discontinued? Why? OR: To become a generic in 1.5 yrs? Provide good illustrations, key references and acknowledgements. Make it fun and special