Download
1 / 1
30 likes | 305 Views
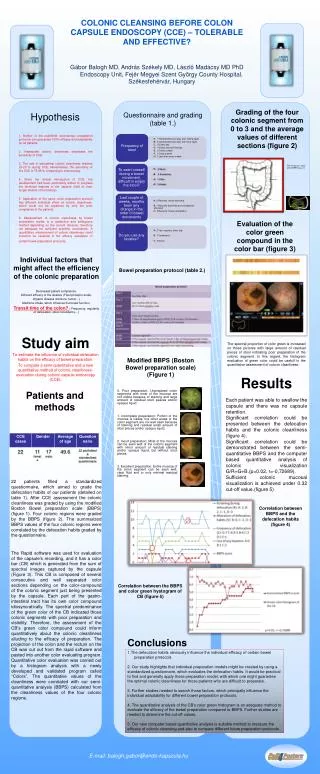
COLONIC CLEANSING BEFORE COLON CAPSULE ENDOSCOPY (CCE) – TOLERABLE AND EFFECTIVE? Gábor Balogh MD, András Székely MD, László Madácsy MD PhD Endoscopy Unit, Fejér Megyei Szent György County Hospital, Székesfehérvár, Hungary.

E N D
COLONIC CLEANSING BEFORE COLON CAPSULE ENDOSCOPY (CCE) – TOLERABLE AND EFFECTIVE? • Gábor Balogh MD, András Székely MD, László Madácsy MD PhD • Endoscopy Unit, Fejér Megyei Szent György County Hospital, Székesfehérvár, Hungary Grading of thefourcolonicsegmentfrom 0 to 3 and theaveragevalues of differentsections(figure 2) Hypothesis Questionnaire and grading (table 1.) 1. Neither of the published colonoscopypreparation protocols can guarantee 100%efficacy and adaptability for all patients. 2. Inadequate colonic cleanliness decreases the sensitivity of CCE. 3. The rate of suboptimal colonic cleanliness reaches 18-20 %during CCE. Nevertheless, the sensitivity of the CCE is 75-89 % comparing to colonoscopy. 4. Since the clinicalintroductionof CCE, the development had been particularly aimed to progress the technical features of thecapsule(field of view, longer lifetime of the battery). 5. Application ofthe same colon preparation protocol has different individualeffectoncoloniccleanliness, which could not be explained by only thepoorcompliance of the patients. 6. Measurement of colonic cleanliness by bowel preparation scales is a subjective and ambiguous methoddepending on the current observer, therefore not adequate for sufficient scientific conclusions. A quantitative measurement of colonic cleanliness could therefore be essential in the efficacy evaluation of certain bowel preparation protocols. The maximum value of the BBPS was 12 Evaluation of the color green compound in the color bar (figure 3) Individual factors that might affect the efficiency of the colonic preparation Bowel preparation protocol (table 2.) Decreased patientcompliance. Different efficacy of thelaxative (Fleetphosphosoda). Organicdisease(stricture, tumor…) Medicine intake, which influence the bowel function. Transit time of the colon? ( Frequency, regularity of defecation, stool consistency…) To estimate theinfluence of individual defecationhabits on the efficacy of bowel preparation. To compare a semi-quantitative and a new quantitative method of colonic cleanliness-evaluationduringcoloniccapsuleendoscopy (CCE). Study aim The spectralproportion of color green is increased on those pictures with large amount of residual pieces of stool indicating poor preparation of the colonic segment. In this regard, the histogram evaluation of greencolorcould be usefull in thequantitativeassessment ofcolonic cleanliness. Modified BBPS (Boston Bowelpreparationscale) (Figure1) Results Patients and methods 0. Poorpreparation: Unprepared colon segments with most of the mucosa are not visible because of staining and large amount of residual stool peaces and/or opaque liquid. 1. Incompletepreparation: Portion of the mucosa is visible, but other areas of the colon segment are not well seen because of staining and residual small amount of stool pieces and/or opaque liquid. 2. Good preparation: Most of the mucosa can be seen well of the colonic segment with minor amount of residual staining and/or opaque liquid, but without stool pieces. 3. Excellentpreparation: Entire mucosa of the colon segment can be seen well, clear fluid and or only minimal residual staining. Each patient was able to swallow the capsule and there was nocapsuleretention. Significant correlation could be presented between the defecation habits and the colonic cleanliness (figure 4). Significant correlation could be demonstratedbetween the semi-quantitative BBPS and the computer based quantitative analysis of colonic visualization G/R+G+B.(p=0.02, r=-0,72689). Sufficient colonic mucosal visualization is achieved under 0.32 cut-off value.(figure 5). 22 patients filled a standardized questionnaire, which aimed to grade the defecation habits of ourpatients (detailed on table 1). After CCE assessment the colonic cleanliness was graded by using the modified Boston Bowel preparation scale (BBPS) (figure 1). Four colonic regions were graded by the BBPS (figure 2). The summarized BBPS values of the four colonic regions were correlated by the defecation habits graded by the questionnaire. Correlation between BBPS and the defecation habits (figure 4) The Rapid software was used for evaluation of the capsule’s recording, and it has a color bar (CB) which is generated from the sum of spectralimages captured by the capsule (Figure 3). This CB is composed of several consecutive and well separated color sections depending on the color-compound of the colonic segment just being presented by the capsule. Each part of the gastro-intestinal tract has its own color compound idiosyncratically. The spectralpredominance of the green color of the CB indicated those colonic segments with poor preparation and visibility. Therefore, the assessment of the CB’s green color compound could inform quantitatively about the colonic cleanliness alluding to the efficacy of preparation. The projection of the colon and the rectum on the CB was cut out from the rapid software and pasted into another color evaluating program. Quantitative color evaluation was carried out by a histogram analysis with a newly developed and validated program called “Colors”. The quantitative values of the cleanliness were correlated with our semi-quantitative analysis (BBPS)calculated from the cleanliness values of the four colonic regions. Correlation between the BBPS and color green hystogram of CB (figure 5) Conclusions 1.The defecation habits obviously influence the individual efficacy of certain bowel preparation protocols. 2. Our study highlights that individual preparation models might be created by using astandardizedquestionnaire, which evaluates the defecation habits. It would be practical to find and generally apply those preparation model, with which onemightguarantee the optimal colonic cleanliness for those patients who are difficult to preparate. 3. Further studies needed to searchthose factors, which principally influence the individual adaptabilityfor differentbowel preparation protocols. 4. The quantitative analysis of the CB’s color green histogram is an adequate method to evaluate the efficacy of the bowel preparationcomparedto BBPS. Furtherstudiesareneededtodeterminethecut-offvalues. 5. Our newcomputer based quantitative analysis is suitable methodto measure the efficacy of colonic cleansing and also to comparedifferent future preparation protocols. E-mail: balogh.gabor@endo-kapszula.hu