Download
1 / 41
420 likes | 611 Views
Z Score Neurofeedback for Insomnia. A New Look at an Old Workhorse: Sensorimotor Neurofeedback.

E N D
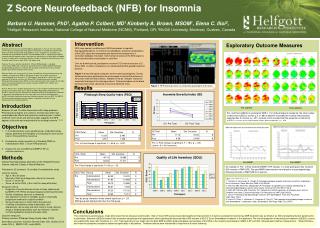
Z Score Neurofeedback for Insomnia A New Look at an Old Workhorse: Sensorimotor Neurofeedback
Barbara U. Hammer, Ph.D., Agatha P. Colbert, M.D., Kimberly A. Brown, MSOM, Helfgott Research Institute, National College of Natural Medicine, Portland, OR, Elena C. Ilioi, Psychology Honours, McGill University, Montreal, Quebec, Canada, The authors wish to thank the Helfgott Research Institute of the National college of Natural Medicine for its support of this research, and William L. Gregory, Ph.D. for providing our statistical analysis. We appreciate of the generous time, energy, and support provided by our Research Assistants who helped in the development and conduct of the investigation: Sean E. Griffith of the Psychology Department at Duke University and Tineke Malus of the Natural College of Natural Medicine. This study was not supported by any industry funding.
2005 NIH Conference on Insomnia declared Insomnia an Epidemic: • 10-20% of adults, mostly Women & Seniors, have Insomnia • Another 20-40% report sleep disturbances • 40% of children, especially those with other vulnerabilities
National Sleep Foundation--November, 2009 • 27% say their sleep has been disturbed at least a few nights a week in the past month due to personal financial concerns (16%), the U.S. economy (15%), and/or employment concerns (10%). • 54% of those losing sleep over economic concerns also had difficulty with their feelings at least a few days a week in the last month. • People with sleep problems are sleeping less than 6 hours on a typical workday or weekday (35% vs. 14%); and/or • They say they’ve driven drowsy at least once a month in the past year (41% vs. 23%). • Problems resulting from Insomnia are increasing
National Sleep Foundation 2009 poll: Effects on Health and Daytime Funcitoning: Compared to their better sleeping counterparts, these people are more likely to report being unable to do the following because they are too sleepy: o Work well and efficiently (25%) o Exercise (30%) o Eat healthy (22% ) o Have sex (16% ) o Engage in leisure activities (28% )
more Effects on Health: • Memory formation impairment=long-term memory impairment (Buzsaki, Sept.,2009) • Additional health care costs up to $14 billion (NSF) • Sleepy drivers =major public safety problem & cost(NSF) • Higher work place accident rates & lost productivity estimated $80 billion (NSF) • Reduced immunity if Sleep Efficiency <92% (Cohen, Oct., 2009)
October, 2009 (Cohen, 2009) found immunity to rhinovirus correlated with the amount of sleep in healthy adults. 1. Graded association with average sleep duration: participants with <7 hours of sleep were 2.94 times (95% confidence interval [CI], 1.18-7.30) more likely to develop a cold than those with 8 hours or more of sleep. 2. The association with SE was also graded: participants with less than 92% efficiency were 5.50 times (95% CI, 2.08-14.48) more likely to develop a cold than those with 98% or more efficiency
Insomnia Definition Primary Insomnia (DSM 307.44): Complaints of Difficulty Falling Asleep, Staying Asleep or Awakening too early, or Non-restorative Sleep which occurs for at least one month duration and: 1. Causes significant distress or impairment in social, occupational, or other important areas of daytime functioning. 2. Does not occur exclusively during the course of Narcolepsy, Breathing-Related Disorder, Circadian Rhythm Sleep Disorder or a Parasomnia. 3. Does not occur exclusively during the course of another mental disorder. 4. Is not due to the direct physiological effects of a substance or general medical condition.
Definition of Insomnia Most Widely Used • In Clinical Practice (American Board of Family Practice) and often in Research: • Sleep Latency (SOL) >30 minutes • Sleep Efficiency (SE) <85% • Sleep Disturbance >3 times a week • Research (Sleep, 2006, April: 29(4)) suggests cutoff of 20” is most sensitive and specific.
TREATMENTS: • Pharmaceuticals • Benzodiazepines most widely used, cannot use long term • Hypnotics can also cause Depression • Reports often hide drug harm (Lunesta, Rozerem) • CAM: • In 2007, 4.5% (1.6 million) of those surveyed used CAM treatments for Insomnia. Summary from NCCAM website November, 2009:
CAM • Herbal products studied lack demonstrated evidence of effectiveness: • Valerian, Melatonin, Chamomile, Kava, 5-HTP, & L-tryptophan (may be harmful, banned) • Aromatherapy-some sleep inducing effects
OtherCAM • Acupuncture-inconclusive. New RCT shows promising results, from 270” electroacupuncture. Only slight but sign. difference pre vs post Rx in SE from Diaries and from Actigraph. • Meditation, yoga-inconclusive. Just completed, unpublished RCT : daily Kundalini, just prior to bedtime, 8 wks>sign. reductions in severity. • Relaxation techniques—EMG Biofeedback etc= mixed/inconclusive. Unpublished study showed SMR >EMG
Psychological treatments • highest co-morbidity • Insomnia persists despite psychotherapy for depression or anxiety • Physiological hyperarousal hypothesis-some support • Cognitive Behavior Therapy—DemonstratedEfficacy • Sleep Restriction • Stimulus Control • difficult to administer • New Internet based program promising
1976, Hauri et al: Waking SMR correlated +.64 with SE & -.64 with SOL 1981, Hauri et al: Compared EMG & Theta & SMR biofeedback Only SMR significantly improved Sleep Tense Insomniacs benefited from Theta BFD
September, 2008 aapb: Peter Hauri (Mayo Clinic): SMR Neurofeedback in 1980’s used Analog Equipment not feasible for general clinical use: Too Expensive Too Cumbersome Too Time consuming “Time to revisit SMR for Insomnia with Digital equipment and new training methods.” This was the exact purpose of our study, which had been given IRB approval just the previous month-in August, 2008!
Overview: Purpose–Compare effectiveness of SMR NFB and (a sequential, quantitative EEG) an EEG guided (IND) protocol for amelioration of Insomnia Methods –RCT single-blind study. Intervention –Groups received 15 20-minute sessions of Z-Score NFB. Pre-post measures –Mental health (MMPI-2-RF and PDSQ), Quality of Life Index (QOLI), Insomnia Severity Index (ISI), Pittsburgh Sleep Quality Index (PSQI), sQEEG.
Neurofeedback Background & Rationale: 2 Primary Approaches Reflected in our 2 Groups 1. Symptom Based: Early SMR Othmers’ 1980’s 2. 2-19 Channel QEEG/Brain Map Guided Lubar Walker Ayers
PARTICIPANTS: 20+ Telephone Screening –unpaid, recruited over 4 months Exclusions—use of sleep aids, psychotropic meds, mental or physical disorders that could interfere, prior NFB, enrolled in another sleep study, pregnant 15 Passed Telephone Screening 12 Invited to enter study 2 Declined to start- personal/extraneous reasons 2 Dropped out- personal/external reasons ≤8 visits
Figure 1: Demographics, Complaints, & Scores • Age Sex Problems PreISIPostISIPrePSQIPosPSQI Duration Group • F WASO,WE 18 5 14 3 Childhood SMR • F SOL,WASO,WE 28 7 17 5 Childhood SMR • F WE,SOL 12 7.5 11 5 22+ yrs IND • F WE,WASO,SOL 14 6 9 4 20+ yrs IND • 50 F WASO 15 9 11 5 1-5 yrs SMR • M NS,WASO,WE 14 9 12 5 10+ yrs IND • M SOL,WASO,WE 19 8 17 6 5 yrs SMR • M SOL,WASO 17 1 16 3 1 yr SMR • Insomnia/Sleep Disturbance Cutoffs =8= ISI 5=PSQI • Pre Average: ISI= 17.13 PSQI= 13.38 • Post Average: ISI= 6.56 PSQI= 4.5
MEASURES continued MMPI-2 RF--Most widely researched, used measure of psychopathology. Newest version Psychiatric Diagnostic Screening Questionnaire- PDSQ—Guide to depth clinical interview to confirm absent Dx Quality of Life Index-QOLI—Measures positive mental health=daytime function Actiwatch--Records movement/lack of movement. 3 days pre vs post. Multiple technical difficulties prevent use of data.
MEASURES continued • sQEEG—sequential EEG—EEG Screening • Records several minutes at 4 scalp sites in succession in 5 runs • Records connectivity measures between each set of 4 sites • Certified Calibration tested EEG amplifier for NFB/sQEEG for FDA
METHODS: • NFB=Operant Conditioning to Norm • Training to Norm =Normalizing physiological process via self-regulating brainwave distribution • Based on Principles of Learning via Reinforcement • Need to monitor progress continually • Z Score NFB designed to use Live, Instantaneous record as basis of Reinforcement
Z Score Neurofeedback Physiological training toward Norm Z=0
Results Insomnia Severity Index • PR = pre, PO = post • Age and Gender were not significant and did not interact with anything so dropped • Pre to Post Change Test F(1,6) = 18.2, p < .005
There is a hint of an interaction, p < .18, change differs between the treatment groups. The IND group does not change as much as the SMR group. It suggests IND is certainly not better than SMR, and it may be the other way around.
PSQI Pre to Post treatment Time change is sig, F(1,6) = 55.6, p < .0001.Covariates not significant
PSQI Time by group interaction is marginally significant, F(1,6) = 4.5, p < .08. SMR is better.
PSQI Sleep Efficiency Pre to Post Change over time is sig, F(1,6) = 15.8, p < .007. Covariates not significant
PSQI Sleep Efficiency No interaction with treatment. No treatment is better than the other.
QOLI: Pre to Post Time change is significant, F(1,6) = 9.6, p < .02. Covariates not significant
Pre to Post Time by group interaction tends toward sig, p < .23. SMR slightly better.
QEEG Abnormal Waves Pre PostSignificance Delta 107 42 p<.001 Beta 54 33 p<.01 Hi Beta 21 17 p<.11 Delta: Pre to post changes 107/304 vs 42/304 yields Z =6.0, p < .001, signif. Beta: Pre to post 54/304 vs 33/304 yields Z = 2.6, p < .01, significant Hi Beta: Pre to post not significant, p < .11, not significant
MMPI-2-RF: Pre vs Post Changes in Borderline Profile -004 Overall T score: Pre=54.11, Post=50.56. Three excessive Scale scores reduced to Normal: Demoralization, Dysfunctional Negative, Aberrant Ex
MMPI-2-RF: Pre vs Post Changes in Borderline Profile -010 Overall level Pre=73.3, Post=50.22 yielding >23 pt. reduction=very significant statistically & clinically
Actiwatch • Multiple Technical Difficulties Prevent Analysis • Click sound inaudible • Possibly Defective recording hardware • and software • Corrections of data with Sleep Log questionable • Participant errors • Processor errors
Summary of Results: • Total Scale scores Significant on both Insomnia Measures: ISI=p<.005, PSQI=p<.0001 • PSQI Sleep Efficiency improved significantly p<.007 • QOLI improved significantly <.02 • Slight but not significant tendency for SMR to be better than IND. • Abnormally high levels of Delta and Beta power at Baseline p<.001 • Delta and Beta power were significantly lowered post-treatment p<.001 Baseline HiBeta amplitude was not excessive. • MMPI-2-RF, borderline-normal subjects showed post-treatment clinical improvement.
Conclusions: • Baseline EEGs showed both excessive sleepiness and hyperarousal, which significantly improved post-treatment. • Both NFB protocols provided significant improvement in self reported sleep and daytime functioning. • Some tendency for SMR treatment to be more effective than IND, and it was significantly less burdensome to administer. • No adverse events reported from full treatment
Discussion • Data replicates early SMR studies with new equipment and advanced software/training designs • Z score NFB possibly effective after <15 Rx sessions (≤300”) • SMR may be more effective than Individually designed protocol based on sQEEG • All participants improved on ALL self-report sleep measures • The power of Z Score SMR NFB suggest it could be very useful for the general Insomnia population
Discussion (continued) 5) sQEEG improvement demonstrates daytime physiological normalization 6) All subjects tolerated 9 weeks of Z Score NFB 7) 15 sessions of NFB safe 8) Non-Invasive, non-pharmacological 9) SMR Easily replicated and practical for clinic use 10) Robust effects 11) QEEG or sQEEG may offer useful Biomarkers for Insomnia