Download
1 / 23
240 likes | 310 Views
Explore the genetic and molecular aspects of epigenetic alterations in cancer, including loss of heterozygosity and gain of function. Learn about key therapies, treatment options, and clinical trials for myelodysplastic syndromes and acute myeloid leukemia.

E N D
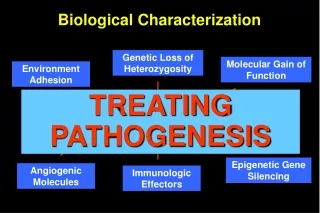
Genetic Loss of Heterozygosity Molecular Gain of Function Environment Adhesion MDS phenotype Epigenetic Gene Silencing Angiogenic Molecules Immunologic Effectors Biological Characterization TREATING PATHOGENESIS
Alteration of the heritable state of gene expression causing disruption of gene function (loss of function), in cancer Gene silencing mediated by: DNA methylation (DNA Methyltransferase) Histone de-acetylation (Histone deacetylase) RNA interference (post-transcriptional) MicroRNA Epigenetic events reversible Potentially targets for cancer therapy (gene reactivation) EPIGENETICS
S t r a t i f y R a n d o m i z e Exit Criteria 1) Supportive Care* RA RARS RAEB RAEB-T CMML + Yes Aza C(dose as per arm #2) A S S E S S • Response • Continue Rx • No Response • - Off Study 2) Aza C75mg/m2/d x 7 days q28 x 4 QOL QOL QOL M M M 0 29 57 113 Day * Minimum duration of supportive care = 4 months unless transform to AML; death or pltsš 20 x 109/L at week 8 or later QOL – Quality of Life Assessment M = Bone Marrow Aza C – Azacitidine S.C. Silverman L, et al. J Clin Oncol 2002. 18:2414-26. Kornblith AB, et al. J Clin Oncol 2002. 18:2427-39 CALGB 9221A Randomized Phase III Controlled Trial of SubcutaneousAzacitidine in Myelodysplastic Syndromes Continue untilEndpoint + No
SC AZA Crossover • No. Evaluated 92 99 49 CR 0 (0%) 7 (7%)* 5 (10%) PR 0 (0%) 15 (16%) ** 2 ( 4%) Improved 5 (5%) 38 (37%) ** 16 (36%) Total 5 (5%) 60 (60%) ** 23 (47%) P - value * < 0.01 **<0.001 Silverman L, et al. J Clin Oncol 2002. 18:2414-26. Analysis of Response
1.0 + + + + + + + + 0.8 + + + Azacitidine Supportive Care 0.6 + + + + + + + + + + Probability of Remaining Event-Free + 0.4 + + + + + + + + + + + + + + + + + + + + + + + + 0.2 + + + + + + 0.0 P=.001 0 6 12 18 24 30 36 42 48 54 Months p=0.007 Time to AML Transformation Silverman L, et al. J Clin Oncol 2002. 18:2414-26.
Azacitidine Supportive Care 1.0 1.0 0.8 0.8 Probability of Survival Induction Azacitidine 0.6 0.6 Crossed before 6 months Did not cross before 6 months 0.4 0.4 0 6 12 18 24 30 36 42 Probability of Survival 48 54 0.2 0.2 Months p=0.1 0.0 0.0 0 5 10 15 20 25 30 35 40 45 50 Months p=0.03 Silverman L, et al. J Clin Oncol 2002. 18:2414-26. Survival
1.0 Aza/Low Supp Care/Low 0.8 Aza/High Supp Care/High 0.6 Probability of Survival 0.4 0.2 0.0 50 40 30 20 10 0 Months Silverman L, et al. J Clin Oncol 2002. 18:2414-26. Survival: FAB Classification
Confirmatory Trial Design Azacitidine 75 mg/m2 x 7 days Every 28 days Patient Randomized Standard of care vs Standard of care Options Options 1) 1) Best Supportive Care Best Supportive Care 2) 2) Low Dose Low Dose Ara-C 3) 3) Standard Chemotherapy Standard Chemotherapy Primary endpoint: Time to leukemic transformation or death
135mg/m2, c.i./72 h 15 mg/m2, tid/Dx3, i.v. 15 mg/m2, tid/Dx3, s.c. Low Dose DAC Kantarjian, Blood 2006
Cumulative analysis of 177 MDS patients treated with low-dose decitabine within 4 Phase II studies in Europe and the USA (Wijermans, Lübbert et al., Ann. Hemat. 2005)
170 pts, DAC 15 mg/m2, tid/Dx3 Q 6 wks, 10 cycles IPSS No. DAC SC P Int-2 74 12 6.8 0.028 HR 44 9.3 2.8 0.01 All pts 170 12.1 7.8 0.16 Report of Phase III Trial of Decitabine in advanced MDS Median time to AML or death (months)
Time to AML P=0.16
Time to AML P=0.028
AZACITIDINE + PHENYLBUTYRATE AZACITIDINE + SAHA (Vorinostat) AZACITIDINE + MS-275 AZACITIDINE + Gemtuzumab Ozogamicin DECITABINE + VALPROIC ACID Combination Therapy for MDS/AML
CANDIDATE DRUGS FOR EPIGENETIC THERAPY DNMT inhibitorsVidaza, Dacogen, zebularine, DNMT antisense and siRNA HDAC inhibitors
Pharmion Corp. MethylGene Taiho HDAC programme • MGCD 0103 • Profile: • HDAC1,2,3 and 11 inhibitor • Oral • Lacks cardiac toxicity (Herg channel negative) characteristic of the class. • Appears synergistic with Vidaza
# Patients Status 3-week cycle Closed 001 Ph I solid 12 002 Ph I solid 28 56 mg/m2 70 mg/m2 003 Ph I – MDS, leukemia 23 53 mg/m2 3 004 Ph I – MDS, leukemia 3 005 Ph I/II – azacitidine combo MDS 90 mg total At sites 0 006 Ph I/II – gemcitabine combo pancreatic 007 Ph II – AML 0 Underway 008 Ph II – Lymphoma 0 Underway MG-0103 Clinical Studies in Cancer
MG-0103 Clinical Studies in Cancer When the highly promising Vidaza,ATRA, Valproate studies in HR MDS/AML and Phase II MGCD0103 studies are completed 0103 will progressively replace valproate
Treatment of BCL6-expressing Burkitt lymphoma cells with cambinol (Sirt1 inhibitor) induced apoptosis, accompanied by hyperacetylation of BCL6 and p53. Acetylation inactivates BCL6 and activates p53 and other checkpoint pathways* *Heltweq, Cancer Res, 2006 HDAC class3 Sirtuins