Abstract
10 likes | 157 Views
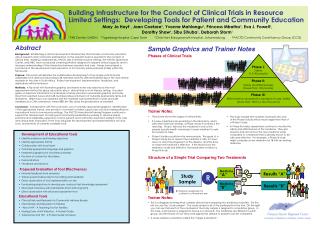
Phase I: Safety (15–30 people) Phase II: Safety and Effectiveness (Fewer than 100 people) Phase III: Effectiveness compared to standard of care; Safety (More than 100 to a few thousand).

Abstract
E N D
Presentation Transcript
Phase I: Safety (15–30 people) Phase II: Safety and Effectiveness (Fewer than 100 people) Phase III: Effectiveness compared to standard of care; Safety (More than 100 to a few thousand) Building Infrastructure for the Conduct of Clinical Trials in Resource Limited Settings: Developing Tools for Patient and Community Education Mary Jo Hoyt1, Joan Coetzee2, Yvonne Mahlangu3, Princess Mbatha3, Eva J. Powell4, Dorothy Shaw4, Sibu Sihuba2, Deborah Storm1 1 FXB Center, UMDNJ 2 Tygerberg Hospital, Cape Town 3 Chris Hani Baragwanath Hospital, Johannesburg 4 PACTG Community Constituency Group (CCG) Abstract Background:Establishing a clinical and research infrastructure that includes community education about research and community participation on the research team is essential to the conduct of clinical trials. Working collaboratively, PACTG sites in limited resource settings, the PACTG Operations Center, and FXBC have conducted a training initiative designed to expand clinical capacity and to increase understanding of the intersection between research and care. Nurses have played a pivotal role in the development and education of Community Advisory Boards (CABs) within this framework. Purpose:This poster will describe the collaborative development of two simple, practical and adaptable tools aimed at educating CAB members and HIV affected families about HIV and clinical research at two sites in South Africa. Project development, implementation, feedback, and implications will be reviewed. Methods:A flip chart with illustrative graphics and trainer notes was selected as the most appropriate method for group education about clinical trials in a low literacy setting. A pocket guide on basic HIV information for individual or family education used similar graphics and notes. Input from selected nurses and CAB members allowed inclusion of culturally appropriate terms and illustrations. Wider input was obtained with the materials were presented to nurses and CAB members at a CAB conference, where 88% (N=156) rated the presentation as excellent. Conclusion: Collaboration with the local team, use of culturally appropriate graphics, identification of the appropriate format, and provision of content for trainer support are crucial in making effective educational tools for low-resource settings. The PACTG International Training Program continues to support the development of nursing and community leadership by working to develop simple, practical and adaptable supportive tools for patient and community education related to HIV care and clinical trials. Evaluation of the tools will guide the development and implementation of future tools, and revisions of currently available tools. Sample Graphics and Trainer Notes Phases of Clinical Trials Trainer Notes: • This picture shows the stages of clinical trials. • If a new medicine looks promising in the laboratory, and is safe when tested in animals, a Phase I study in humans is the next step. Phase I trials test the medicine in only a few people (usually health volunteers) to learn whether it is safe for humans to take. • Phase II studies usually involve more people. The goals of a Phase II study are to assess if the medicine is safe, if it slows down or stops the progression of the disease, and the dose at which the medicine is effective. If the results show the medicine is safe and effective, the researchers conduct a Phase III study. • The study sample (the number of people who join) of the Phase III study will be much larger than that of a Phase II study. • In Phase III studies, researchers continue to monitor the safety and effectiveness of the medicine. They also observe and record how the new medicine works compared to a medicine that is already known to be safe and effective. For example, a Phase III study might compare a new medicine for TB with an existing medicine. • Development of Educational Tools • Identify audience and training objectives • Identify appropriate format • Collaboration with local team • Culturally appropriate language and graphics • Interpretive graphics for low-literacy learners • Provision of content for the trainer • Demonstrations • Feedback and revisions Proposed Evaluation of Tool Effectiveness • Informal feedback from reviewers • Trainer questionnaires rate for tool rating and feedback • Direct observation of tool implementation on-site • Use learning objectives to develop pre- and post-test knowledge assessment • Structured interviews with participants (short and long term) • Direct observation with structured assessment tool Educational Tools • Clinical Trials and Research for Community Advisory Boards • Clinical Trials and Research for Families • “About HIV” A Teaching Tool for Families • Nursing Care of HIV Infection: A Pocket Guide • Tuberculosis and HIV: A Pocket Guide for Nurses Structure of a Simple Trial Comparing Two Treatments Medicine “A” Results “A” Study Sample R Medicine “B” Results “B” R = Random assignment of patients to a treatment arm Trainer Notes: • This is a diagram showing what a simple clinical trial comparing two medicines looks like. On the left you see the “study sample”. The study sample is all of the participants in the trial. On the right you can see that each of the volunteers in the study sample is assigned to a medicine group. In this case, each person is assigned to Group A or Group B. The medicines are different in each group, and the results of how they work against the disease or problem can be compared. • A study sample is sometimes called the “target population”.


















