Download
1 / 54
540 likes | 702 Views
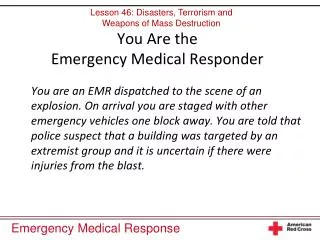
Emergency Responding to the Emergency Responder. Stress, Coping and Surviving in the Emergency Services. Officer Joel Fay Psy.D (415) 720-6653 Joel.Fay@SRPD.0rg. Post Traumatic Stress Disorder – An Assault on the Mind, Body and Spirit. PTSD. PTSD is a total person experience Symptoms effect

E N D
Emergency Responding to the Emergency Responder Stress, Coping and Surviving in the Emergency Services Officer Joel Fay Psy.D(415) 720-6653 Joel.Fay@SRPD.0rg
Post Traumatic Stress Disorder –An Assault on the Mind, Body and Spirit
PTSD • PTSD is a total person experience • Symptoms effect • Mental Health • Physical Health • Family and Friends • Work • Spirit
PTSD – Diagnostic Criteria Must be exposed to a traumatic event Person's response to the event must involve intense fear, helplessness, or horror
The event must be re-experienced by distressing recollections, dreams, flashbacks, etc.
Avoidance of locations, persons, etc • Sense of isolation • “No one else knows what I am going through” • “I can’t burden other people with this.”
Persistent Problems With Increased Arousal • Withdrawal • Irritability • Insomnia • Hyper-vigilant
Symptoms of the Spirit • Hopelessness • Helplessness(Locus of Control) • Meaning of life • Questioning faith
How The Brain Processes Threats And why it’s NOT our Fault
How It Works • Thalamus – is a routing station for all incoming sensory impulses except smell
How It Works • Thalamus – Routes information from eyes and ears to the brain
Amygdala • Small almond shaped structure near the middle of the brain. • Attaches meaning to memory • Places the experience into the context of an emotion.
The Amygdala is the command center of the brain’s fear system.
Brain’s Response • Works with Hippocampus by evaluating threats and placing them in the context of a previous experience. • Prefrontal Cortex – Reins in the Amygdala if the threat is deemed to be insignificant.
What Happens Next? • Amygdala – If threat is sufficient the body shuts down non-emergency services (I.e., digestion and immunity) • Triggers body wide emergency response within seconds
Hypothalamic-Pituitary-Adrenal System (HPA) • Release of Cortisol to activate the bodies defense systems • Release of Catecholamines -dopamine, norepinephrine, and epinephrine
Catecholamines • Suppress activity in areas at the front of the brain concerned with short-term memory, concentration, inhibition, and rational thought. • This allows a quick reaction to the threat
What is Memory? The use of past experiences to affect future behavior.
Heightened alertness in the brain – which in effect tells the memory centers, “Remember what occurred.”
Although cognitively you know that the event is over, part of you (your nervous system) still feels that the event is happening. This constant state of alertness taxes your body and spirit.
“What makes an incident Critical?” • Perceived threat / trauma • Your body’s reaction • What else is happening in your life • The meaning you attribute to an event
EVENT “Once you crossed over that line – there is no going back.”
Stress vs. Critical Incident Stress • Daily stress • Stress v. Distress
Organizational/ PersonalBetrayal “It’s about the system” How a person recovers from trauma depends on the support system available after an event. “Don’t punish the victim.”
How Do We React to Trauma • “I think I am going crazy” • “There is something wrong with me.” • “My inability to control my symptoms shows how weak I am” • Fearing Fear – The anticipation of experiencing the symptoms can be almost as debilitating as the symptoms themselves.
How Do We React to Trauma We have trouble controlling emotions because reminders lead to sudden anxiety, anger, or upset • We feel anger or aggressive feelings and feel the need to defend ourselves • We get upset when we are reminded about the trauma (by something the person sees, hears, feels, smells, or tastes)
You cannot predict and you cannot control your life to the extent that would make you feel comfortable and safe. To adjust to this lack of control – you check out, numb yourself become unavailable.
The Cost of Denying Emotions • In 2002, 437 paramedics were tested to look at long term effects of suppressing emotions. • The greater the emotional suppression – the greater the physical and psychological stress symptoms. Wastell, 2002
Our strengths are the other side of our weaknesses Self- Control – Physical and Psychological Not affected by what we experience Command presence
Commonly Used Maladaptive Coping Techniques • Harder, Faster, Better • Hyper-Activity • Counter Phobic Behavior • Impulsive and Reckless Behavior w/o Thought
Commonly Used Maladaptive Coping Techniques • Multiple Romantic Relationship • To obtain positive mirroring • “I can’t be bad, look how much she loves me”
More… • Overcompensation • Token attempts seeking professional help. • Alcohol / Substance Use
What These Coping Strategies Have in Common • An attempt to recapture the ability for denial • They work – for a while – for some • They are avoidance techniques • They do not include conscious grappling with the issues and fears generated by Cognitive Dissonance
Often the symptoms of a stress reaction are misdiagnosed by supervisors, families, doctors and the individual. Anger, Somatic Reactions, Frustration, Burn Out Person Self-Blame Guilt Second Guessing
The Aftermath of Failed Repaired Efforts • Each failed attempt at restoring the Self-Concept further “proves” fraudulence • Isolation • From work, friends, family and prior activities. • Occurs because there are fewer and fewer people you can reveal one’s self to. • There is a fear of being found “fraudulent”
What Do We Do? AVOIDANCE • Alcohol/ Drugs • Thought Suppression • Risky Behavior • Excess Work This works until it doesn’t
The Aftermath of Failed Repair Efforts • Panic Attacks • Fear of Fear • Self-Blame and Self- Guilt • Depression • Psychic Exhaustion • Global Negative Self Appraisal • Job Site Becomes Toxic Emergency Responder Exhaustion Syndrome
Survival What Can You Do?
Peer Goals • Provide acceptance, validation and empowerment • Breaks the fallacy of uniqueness by demonstrating that they are not alone and that what they are experiencing is normal
Peer Goals • Help clients cope with the myth of invulnerability which has been shattered • Provides hope
Police Chaplains International Conference of Police Chaplains
EAP • Are they culturally competent? • Do you have a list of clinicians you could call on in case of an emergency? • Create a program where local clinicians go on ride-a-longs, do FATS, etc
Who Attends WCPR • Police, fire and emergency services personnel are the typical residents. • People affected by the CI for whom a debriefing or individual therapy has not been sufficient to reduce symptoms. • Most clients come because they are in crisis and “not coming” was not an alternative.
Why Residential Treatment ? • Program must be of sufficient impact / relevance to effectively challenge long held faulty self-concepts. • Robust peer-support network. • VERY culturally competent mental health professionals. • A true collaboration which is peer driven and clinically informed.
Primary Goals • Keep the person alive / Do no harm • Restore psychological and emotional functioning • Reduction of physical symptoms • Restore ability to participate in their own recovery • Link client to appropriate resources
Program Components • Initial Phone Intake • Intake – First, Worst and Last, DAPS • 5 CISD Phases • Education Modules • Family/Relationship Debriefings • Individual / Group* • EMDR • Chaplain • AA • 90 Day Relapse Prevention Plan
Some Data • Gender: 75% male • Substance Abuse Issue: 43.7% Yes • How They Came: • 29% Worker’s Comp • 13% Department Training Funds • 28% - Self Pay • 20% - Scholarships • 6% - Donations (Police Associations)