
ABSTRACT
Carbapenem Activity Against Acinetobacter calcoaceticus-baumanii complex (ACBC) in an In Vitro Pharmacokinetic Bacteremia Model (PKM) Eric G Sahloff, Pharm.D., Diane M. Cappelletty, Pharm.D., & Steven J. Martin, Pharm.D., BCPS, FCCM

ABSTRACT
E N D
Presentation Transcript
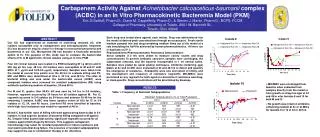
Carbapenem Activity Against Acinetobacter calcoaceticus-baumanii complex (ACBC) in an In Vitro Pharmacokinetic Bacteremia Model (PKM) Eric G Sahloff, Pharm.D., Diane M. Cappelletty, Pharm.D., & Steven J. Martin, Pharm.D., BCPS, FCCM College of Pharmacy, University of Toledo, 2801 W. Bancroft St., Toledo, Ohio 43606 Each drug was tested alone against each isolate. Drug was administered into the model at desired peak concentrations through an access port. Fresh sterile medium pumped into and drug-containing medium flows out of the model at a rate simulating the half-life achieved by human pharmacokinetics. All were run in duplicate at 37o C. Pharmacokinetic/Pharmacodynamic Resistance Determinations Serial samples (1.0 ml) were drawn to measure colony counts and drug concentrations To prevent antibiotic carryover, samples were centrifuged, the supernatant removed, and the bacteria resuspended in 1 ml normal saline. Samples were plated by spiral plating techniques. Antibiotic-containing agar plates at 2x and 4x MIC were evaluated at 24 and 48 hrs to detect and quantify the emergence of resistance. Endopoints were rate and extent of killing, and the development and frequency of resistance (regrowth). MIC/MBCs were performed on any regrowth for both agents to determine if resistance was drug- or class-specific. Drug concentrations will be determined by bioassay. ABSTRACT Our ICU has experienced an outbreak of multi-drug resistant AC, with isolates susceptible only to carbapenems and aminoglycosides. Imipenem (IC) has become an empiric choice for therapy in nosocomial pneumonia and bacteremia in our ICU. Meropenem (M) has become a financially attractive option to IC. The purpose of this study was to compare the bactericidal effects of IC to M against AC clinical isolates using an in vitro PKM. Four AC clinical isolates were tested in a PKM simulating M 1 g q8 hrs and IC 500 mg q6 hrs over 48 hrs. All isolates were susceptible to M and IC with MICs of 1 g/ml and 0.25-0.5 g/ml, respectively. Samples were taken from the model at several time points over the 48 hrs to evaluate killing and PK. MIC and MBCs were determined at time 0, 24 hrs, and 48 hrs. The rates of bacterial killing and area under the bactericidal curves (AUBC) were compared. Isolates were screened for resistant subpopulations (RS) using antibiotic-containing medium at baseline, 24 and 48 hr. For M and IC, greater than 99.9% kill was seen by 3-4 hrs in 3/4 isolates,. However, regrowth occurred by 24 hours for all isolates against M. For IC, regrowth occurred in 2/4 isolates by 24 hours and between 30-48 hrs for the remaining 2 isolates. AUBC was lower (greater extent of kill) for IC in 3/4 isolates at 12, 24, and 48 hours. Low-level RS were identified at baseline, while high-level resistance was noted for regrowth at 48 hr. M and IC had similar rates of killing with both agents being bactericidal in 3/4 isolates. IC had superior duration of bacterial killing compared to M against AC. Despite initial bactericidal activity, significant regrowth occurred for all isolates against both drugs by 48 hours. This suggests carbapenem monotherapy may select for resistant populations or induce resistance and coul lead to potential drug failure. The presence of resistant subpopulations may support the use of combination therapy in AC infections. • MIC/MBC were unchanged from baseline when evaluated from samples directly from the model or from growth on drug-free agar at 24 and 48 hr wfor Isolates 9 and 10 for both M and IC • No growth was noted on antibiotic-containing medium at 2x or 4x MICs for Isolates 9 or 10 at 24 or 48 hrs. RESULTS Table 1. Frequency of Resistant Subpopulations
CONCLUSIONS BACKGROUND Acinetobacter spp. Has been documented as the cause of numerous nosocomial outbreaks and has been associated with increased lengths of stay in the ICU as well as increased mortality in infected ICU patients. In our institution the number of isolates cultured nearly doubled from 1998-2000 compared to 2001 with over one-third being multi-drug resistant. Susceptibility to commonly used antibiotics including cefepime piperacillin/tazobactam, and ampicillin/ sulbactam decreased while imipenem/cilistatin and tobramycin susceptibility remained stable. Antimicrobial resistance makes drug selection difficult. Inappropriate antimicrobial selection can lead to increased mortality, while exposure to broad spectrum antimicrobials is associated with development of resistance. Initial selection of antimicrobials at optimal dosing may have a significant effects on patient outcome antimicrobial resistance. Carbapenems alone or in combination with other antimicrobials are considered to be a therapy-of-choice for Acinetobacter infections. The purpose of this study was to compare the bactericidal effects of imipenem/cilistatin (IC) and meropenem (M) against AC clinical isolates using an in vitro PK bacteremia model. Resistant subpopulations were seen in all isolates for IC and M (Table 1). Both agents provided bactericidal killing against 3/4 isolates. Regrowth occurred earlier for M in 3/4 isolates with IC maintaining killing at or below 2 log for ≥ 30 hours in 2/4 isolates. Despite regrowth occurring, no changes in MIC/MBC or growth on antibiotic-containing media were noted for isolates 9 and 10 for either M or IC. In contrast, MIC/MBC changes did occur with isolates 4 and 7. Tables 2 and 3 describe examples of these changes. For isolate 4, selection of a resistant clone likely occurred leading to regrowth in 3/4 model runs. High level resistance was seen when sampling directly from the model as well as off the antibiotic-containing medium. One of 4 runs did not regrow and may be attributed to lack of selection of a resistant clone. MIC/MBC changes occurring in isolate 7 are more difficult to explain. Selection of a resistant clone explains the regrowth occuring in 5/6 runs. No change in MIC/MBC occurred when evauating growth from the 24 hr drug-free plates. Induction of resistance with the addition of the antimicrobial likely occurred followed by reversion back to the susceptible form with the removal of drug pressure. Highly resistant MICs at 48 hours from samples from the model are expected. Tolerance, low MICs and elevated MBCs, is seen when evaluating growth from the 48 hr antibiotic-containing medium as well as with one run of the 48 drug-free plates. A second example (model C) at 48 hrs. maintained high level resistance despite removal of drug pressure. M and IC had similar rates of killing with both agents being bactericidal in 3/4 isolates. IC had superior duration of bacterial killing compared to M against AC. Despite initial bactericidal activity, significant regrowth occurred for all isolates against both drugs by 48 hours. This suggests carbapenem monotherapy may select for resistant populations or induce resistance and coul lead to potential drug failure. The presence of resistant subpopulations may support the use of combination therapy in AC infections. Table 2. MIC/MBC for Meropenem and Imipenem Against Isolate 4 After Exposure to Meropenem METHODS • Organisms/Susceptibilities. • Four AC clinical isolates were tested. Baseline data collected for M an IC against isolate included: • MIC/MBC by microtiter methodologies following NCCLS protocol. • Ppresence of resistant subpopulations on antibiotic containing plates representing 2x and 4x the MIC. Frequency of resistance = the number of organisms growing on the antibiotic-containing medium divided by number of antibiotic-free agar plates. • In vitro pharmacokinetic/pharmacodynamic model. • Isolates were tested over 48 hours against M and IC in a glass one compartment in vitro PK model emulating a bloodstream infection. Drug regimens and human PK parameters to be simulated include: • 1) Imipenem/cilistatin 500 mg every six hours simulating a peak concentration of 40 mcg/ml and a half-life of 1 hour. • 2) Meropenem 1 gram every 8 hours simulating a peak concentration of 60 mcg/ml and a half-life of 1 hour. Table 3. MIC/MBC for Meropenem and Imipenem Against Isolate 7 After Exposure to Meropenem


















