Download
1 / 9
90 likes | 110 Views
"This condition is an umbrella term and includes conditions as impingement, subacromial bursitis, calcific tendinitis, biceps tendinitis, cuff degeneration, rotator cuff tendinopathy and cuff tear. Specialized tests as Neer , Hawkins , Empty-can test have been shown to help the clinician evaluate the shoulder. Anatomy of the shoulder is also described for reference. Role of imaging as MRI , Ultrasound and X-Ray is cited to help the clinician order further investigations. Management and the role of physiotherapy are discussed- acute tear secondary to trauma should be referred urgently. Addressi

E N D
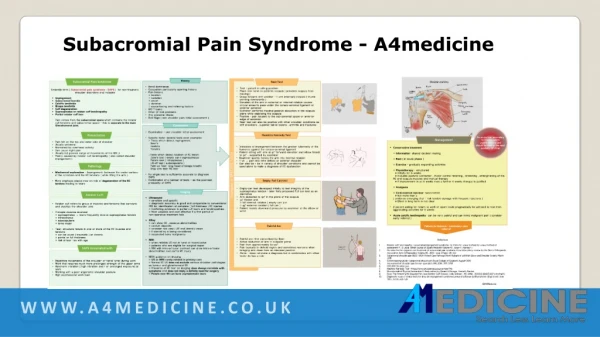
SUBACROMIAL PAIN SYNDROME a4medicine.co.uk
This condition is an umbrella term and includes conditions as impingement, subacromial bursitis, calcific tendinitis, biceps tendinitis, cuff degeneration, rotator cuff tendinopathy and cuff tear. Specialized tests as Neer , Hawkins , Empty-can test have been shown to help the clinician evaluate the shoulder. Anatomy of the shoulder is also described for reference. Role of imaging as MRI , Ultrasound and X-Ray is cited to help the clinician order further investigations. Management and the role of physiotherapy are discussed- acute tear secondary to trauma should be referred urgently. Addressing each condition alone is beyond the scope of this review but a chart with further details is planned on A4Medicine Umbrella term ( Subacromial pain syndrome – SAPS ) for non-traumatic shoulder disorders and includes Impingement Subacromial bursitis Calcific tendinitis Biceps tendinitis Cuff degeneration Supraspinatus or rotator cuff tendinopathy Partial rotator cuff tear Pain comes from the subacromial space which contains the rotator cuff tendons and subacromial space – this is separate to the main Glenohumeral joint Presentation-Pain felt on the top and outer side of shoulder Usually unilateral Worsened by overhead activity Can cause night pain Usually full passive range of movements of the G/H jt Mainly caused by rotator cuff tendinopathy ( also called shoulder impingement )
Pathology-Mechanical explanation – Impingement- between the under-surface of the acromion and the RC tendons ( while lifting the arm ) More emphasis placed now on role of degeneration of the RC tendons leading to tears Rotator -cuff Rotator cuff refers to group of muscles and tendons that surround and stabilize the shoulder joint Principle muscles involved ○ supraspinatus → tears frequently involve supraspinatus tendon ○ infraspinatus ○ subscapularis ○ teres major Tear- structural failure in one or more of the RC muscles and tendons ○ can be acute ( traumatic ) or chronic ○ partial or full thickness ○ risk of tear ↑es with age Presentation-Pain felt on the top and outer side of shoulder Usually unilateral Worsened by overhead activity Can cause night pain Usually full passive range of movements of the G/H jt Mainly caused by rotator cuff tendinopathy ( also called shoulder impingement ) SAPS-Repetitive movements of the shoulder or hand/ wrist during work Work that requires much more prolonged strength of the upper arms Hand-arm vibration ( high vibration and / or prolonged exposure) at work Working with a poor ergonomic shoulder posture High psychosocial work load
Shoulder pain due to SAPS is very common SAPS from RC pathology including tendinopathy , calcific tendinitis and RC tears accounts for up to 70 % of all new shoulder pain problems Annual prevalence of SAP is around 7 % A BMJ paper in 2017 quotes that among shoulder complaints SAP is the most common disorder , representing 89 % of total shoulder complaints referred to GPs and physiotherapists Rotator -cuff Rotator cuff refers to group of muscles and tendons that surround and stabilize the shoulder joint Principle muscles involved ○ supraspinatus → tears frequently involve supraspinatus tendon ○ infraspinatus ○ subscapularis ○ teres major Tear- structural failure in one or more of the RC muscles and tendons ○ can be acute ( traumatic ) or chronic ○ partial or full thickness ○ risk of tear ↑es with age Presentation-Pain felt on the top and outer side of shoulder Usually unilateral Worsened by overhead activity Can cause night pain Usually full passive range of movements of the G/H jt Mainly caused by rotator cuff tendinopathy ( also called shoulder impingement ) SAPS-Repetitive movements of the shoulder or hand/ wrist during work Work that requires much more prolonged strength of the upper arms Hand-arm vibration ( high vibration and / or prolonged exposure) at work Working with a poor ergonomic shoulder posture High psychosocial work load
Shoulder pain due to SAPS is very common SAPS from RC pathology including tendinopathy , calcific tendinitis and RC tears accounts for up to 70 % of all new shoulder pain problems Annual prevalence of SAP is around 7 % A BMJ paper in 2017 quotes that among shoulder complaints SAP is the most common disorder , representing 89 % of total shoulder complaints referred to GPs and physiotherapists Rotator -cuff Rotator cuff refers to group of muscles and tendons that surround and stabilize the shoulder joint Principle muscles involved ○ supraspinatus → tears frequently involve supraspinatus tendon ○ infraspinatus ○ subscapularis ○ teres major Tear- structural failure in one or more of the RC muscles and tendons ○ can be acute ( traumatic ) or chronic ○ partial or full thickness ○ risk of tear ↑es with age Presentation-Pain felt on the top and outer side of shoulder Usually unilateral Worsened by overhead activity Can cause night pain Usually full passive range of movements of the G/H jt Mainly caused by rotator cuff tendinopathy ( also called shoulder impingement ) SAPS-Repetitive movements of the shoulder or hand/ wrist during work Work that requires much more prolonged strength of the upper arms Hand-arm vibration ( high vibration and / or prolonged exposure) at work Working with a poor ergonomic shoulder posture High psychosocial work load
Shoulder pain due to SAPS is very common SAPS from RC pathology including tendinopathy , calcific tendinitis and RC tears accounts for up to 70 % of all new shoulder pain problems Annual prevalence of SAP is around 7 % A BMJ paper in 2017 quotes that among shoulder complaints SAP is the most common disorder , representing 89 % of total shoulder complaints referred to GPs and physiotherapists History-Hand dominance Occupation particularly sporting history Pain history ○ location ○ radiation ○ onset ○ duration ○ exacerbating and relieving factors H/O Trauma Other jt/ msk problems Any systemic illness Red flags ( see shoulder pain initial assessment ) Examination-Examination – see shoulder initial assessment Specific tests- several tests exist examples ○ Tests which detect impingement Neer’s Hawkins Yocum’s ○Tests which detect location of RC lesion Jobe’s test ( empty can ) supraspinatus Patte’s test ( infraspinatus ) Lift-off test ( subscapularis ) Palm-up Test- long head of biceps brachii Drop arm test- RC tear No single test is sufficiently accurate to diagnose SAPS Combination of a number of tests ↑ es the post-test probablity of SAPS
Imaging-not recommended in primary care can be user dependent and the accuracy of reporting can vary a normal US does not mean that serious underlying pathology as tumour and glenohumeral osteoarthritis do not exist a report of partial thickness tear is common and this may be for a patient who is asymptomatic or due to false positive reporting this is more suitable in secondary care setting where the shoulder surgeon can correlate findings in the context of patient symptoms Tests Neer , Hawkins-Kennedy ,Empty can test , Painful arc Management-Conservative treatment ○ Information- shared decision making ○ Rest ( in acute phase ) ○ Exercise – gradually expanding activities ○ Physiotherapy – structured ♦ initially for 6 weeks ♦ includes postural correction , motor control retaining , stretching , strengthening of the RC and scapula muscles and manual therapy ♦ if improvement in 1st 6 weeks then a further 6 weeks therapy is justified ○ Analgesia ○ Corticosterod injection- subacromial ♦ Not more than 2 ( evidence emerging that ↑ risk tendon damage with frequent injections ) ♦ Effect in long term is not clear If patient asking for return to work or sport could pragmatically be advised to rest from aggravating activities for 6 weeks Acute calcific tendinopathy- can be very painful and can mimic malignant pain ( consider early referral ) An acute tear secondary to trauma needs urgent referral and should be seen in the next available OP clinic
MRI- It is largely unknown if the structural changes identified by MRI affect the outcome of non-operative treatment for shoulder pain MRI is often used by shoulder specialists particularly in groups for who a surgical intervention is being considered Referral- any red flag Calcific tendinopathy can be very painful and can often mimic malignant pain – consider an early secondary care referral for more interventional treatment persistent or significant loss of function despite 6 weeks of conservative management Shoulder Pain Disability Index https://www.worksafe.qld.gov.au/__data/assets/pdf_file/0008/77084/shoulder- pain-and-disability-index-spadi1.pdf
References 1. Diercks, Ron et al. “Guideline for diagnosis and treatment of subacromial pain syndrome: a multidisciplinary review by the Dutch Orthopaedic Association.” Acta orthopaedica vol. 85,3 (2014): 314-22. doi:10.3109/17453674.2014.920991 Kulkarni, Rohit et al. “Subacromial shoulder pain.” Shoulder & elbow vol. 7,2 (2015): 135-43. doi:10.1177/1758573215576456 Tangrood ZJ, Gisselman AS, Sole G, et al. Clinical course of pain and disability in patients with subacromial shoulder pain: a systematic review protocol. BMJ Open 2018;8:e019393. doi:10.1136/ bmjopen-2017- 019393 https://bmjopen.bmj.com/content/bmjopen/8/5/e019393.full.pdf Commissioning guide Subacromial Shoulder Pain RCS via https://www.boa.ac.uk/uploads/assets/uploaded/f4bfe04a-0450-4eab-b9acad9dbb5d8c86.pdf Cadogan, Angela et al. “Diagnostic Accuracy of Clinical Examination and Imaging Findings for Identifying Subacromial Pain.” PloS one vol. 11,12 e0167738. 9 Dec. 2016, doi:10.1371/journal.pone.0167738 Kvalvaag, E., Anvar, M., Karlberg, A.C. et al. Shoulder MRI features with clinical correlations in subacromial pain syndrome: a cross-sectional and prognostic study. BMC Musculoskelet Disord 18, 469 (2017). https://doi.org/10.1186/s12891-017-1827-3 ( Abstract ) Vandvik Per Olav, Lähdeoja Tuomas, Ardern Clare, Buchbinder Rachelle, Moro Jaydeep, Brox Jens Ivar et al. Subacromial decompression surgery for adults with shoulder pain: a clinical practice guideline BMJ 2019; 364 :l294 2. 3. 4. 5. 6. 7.