Download
1 / 25
340 likes | 1.05k Views
Anterior Knee Pain Syndrome. James Barsi, MD Assistant Professor of Orthopaedic Surgery June 14, 2013. Anterior Knee Pain Syndrome. Pain with prolonged knee flexion or stairs Vague, localized in peripatellar area. Background. Diagnosis and treatment is challenging

E N D
Anterior Knee Pain Syndrome • James Barsi, MD • Assistant Professor of Orthopaedic Surgery • June 14, 2013
Anterior Knee Pain Syndrome • Pain with prolonged knee flexion or stairs • Vague, localized in peripatellar area
Background • Diagnosis and treatment is challenging • “Anterior knee pain syndrome” groups together different but related pathologic entities
Anterior Knee Pain Syndrome Activity Related Patella tendonitis ITB syndrome Plica syndrome Fat pad syndrome Arthosis Chondromalacia Inflammatory arthritis Constant Pain, not activity related: Sympathetic dysfunction Neuroma Referred radicular pain Secondary Gain Sharp, intermittent pain: Loose bodies Unstable chondral damage Patella Instability Malalignment Syndromes
Pain • Free nerve endings are concentrated in the patella tendon, retinaculum, fat pad1 • Patients with AKPS have perivascular proliferation of nociceptive axons in retinaclum2 • Substance P nerve fibers are widespread within the soft tissues around the knee (retinaculum, synovium, fat pad). In patients with AKPS, more Substance P fibers were found in the fat pad and retinaculum3 (1) Biedert et al. Am J Sports Med 1992; 20: 430. (2) Sanchis-Alfonso et al. Am J Sports Med 1998; 26;703 (3) Witonski et al. Knee Surg Sports TraumatolArthrosc 1999; 7:177-183
Clinical Evaluation • Not all anterior knee pain associated with patella alignment abnormalities • Radiographic findings not pathologic if patient not symptomatic
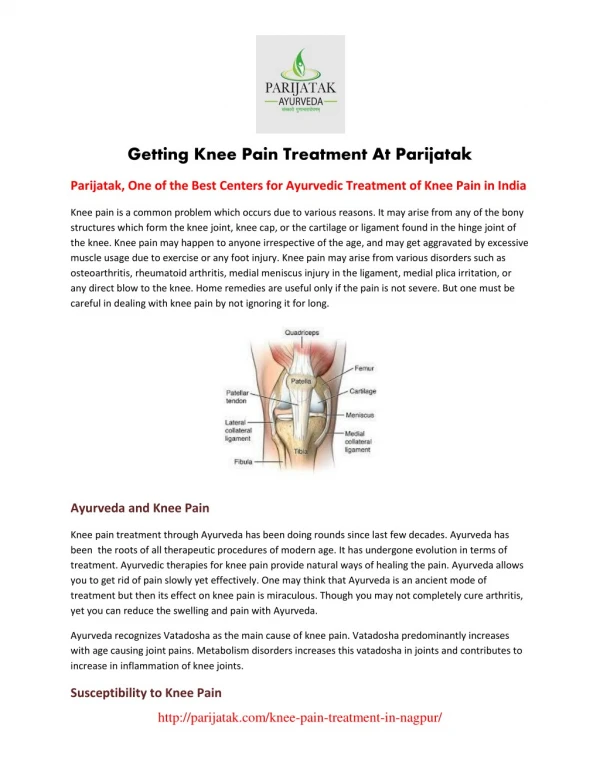
Physical Examination • Observation • Alignment • Varus/Valgus • Rotational • Patella tracking • Pes planus
Physical Exam • Patella apprehension • Tight lateral retinaculum • Quadriceps and hamstring tightness • Hip strength
Radiographs • AP, lateral, Merchant axial view • Patella sitting centered in trochlea • Tilt • Trochlea morphology
Predictors of Pain • 282 adolescents • 10% Patellofemoral Pain • Predictors of developing pain: • Decreased flexion of quadriceps, gastrocnemius • Increased VMO response time • Decreased explosive strength • Increased thumb to forearm mobility 1. Witvrouw et al. Am J Sports Med 2000; 28: 480.
Role of the Hip • Hip extensors absorb 25% energy during landing • Deficits in hip strength add to load on the knee.1 1. Zhang et al. Med Sci Sports Exer 2000; 32: 812.
Nonsurgical Management • Physical Therapy • Knee Brace • Orthotics
Physical Therapy • Traditional concept of trying to achieve isolated VMO strength not supported by literature. • Closed vs open chain: • Both types produced improvements in strength, pain relief and return to function1 1. Witbrouw et al. Am J Sports Med 2000; 28: 687.
Does Physical Therapy Help? • 84% of patients improved after 8 weeks of quadriceps & hip rehabilitation. • 75% of patients maintain improvement 6 months to 7 years2 1. Doucette et al. Am J Sports Med 1992: 20: 434. 2. Kannus et al. JBJS 1999; 81: 355-363
Physical Therapy • Attention should be paid to quadriceps flexibility • Strengthening done without causing pain • Emphasis on hip strengthening • Continued until plateau reached
Surgical Management • Surgery is not necessary in most cases • Successful surgical treatment requires an accurate diagnosis (patella instability or patellofemoral malalignment) • Normal alignment and no instability may be symptomatic from tendinosis in the quadriceps or patella tendons, pathologic hypertrophy and inflammation in the medial plica • Damage to the articular surface may also cause pain
Chondroplasty • Arthroscopic debridement of grade 2 and 3 chondral lesions can be useful • 58% good or excellent results with traumatic onset • 41% good or excellent results with atraumatic onset1 1. Federico et al. Am J Sports Med 1997; 25: 663-669
Lateral release • Effective in treating a well-defined subset of patients • Mechanism • relieves pressure in lateral retinaculum • divides neuromatous nerves in the retinaculum • relieves pressure on the lateral facet of the patella
Lateral Release • Ideal patient • No instability • Tight lateral retinaculum • Outcome related to chondral damage • 59% satisfactory with >grade 31 • 92% good to excellent with < grade 22 1. Aderinto et al. Arthroscopy 2002; 18:399-403 2. Shea et al. Arthroscopy 1992; 8:327-334.
Complications of Lateral Release • Persistent pain • Worsening instability • Suspect medial subluxation in any patient reporting persistent pain after lateral release • Test in decubitus with lateral knee up, patella sags medially from gravity • Patient unable to flex knee
Tibial tubercle transfer • Lateral patellar tilt and subluxation • Results correlated to location of patella chondral lesions • global and proximal lesions did less well • Biomechanical studies show that transfer while decreasing overall load, transfers it disproportionally to proximal patella
Cartilage Restoration • OATS and autologous chondrocyte implantation • Small numbers have been reported and reports are mixed • Less aggressive procedures (chondroplasty, microfracture or abrasion) may be equally effective
Patellofemoral Arthroplasty • Low demand patients • Care at the time of surgery to ensure extensor mechanism is aligned
Summary • Important to establish accurate diagnosis • Non-surgical management remains the most predictable method of treatment