Download
1 / 66
730 likes | 1.18k Views
Non-Alzheimer’s Dementia: What you need to know about Lewy body, frontotemporal, and vascular dementias. James B. Leverenz, M.D. VA Northwest Network Parkinson Disease and Mental Illness Research Education and Clinical Centers

E N D
Non-Alzheimer’s Dementia: What you need to know about Lewy body, frontotemporal, and vascular dementias James B. Leverenz, M.D. VA Northwest Network Parkinson Disease and Mental Illness Research Education and Clinical Centers Departments of Neurology and Psychiatry and Behavioral Sciences, University of Washington School of Medicine Pacific Northwest Udall Center UW Alzheimer’s Disease Research Center
Overview • Dementia & Alzheimer’s disease • Epidemiology, pathology, clinical • Dementia with Lewy Bodies/Parkinson Disease Dementia • Vascular dementia • Frontotemporal dementia
Prevalence of Alzheimer’s Disease 70 60 50 40 Alzheimer’s Disease (%) 30 20 10 0 65 70 75 80 85 90 Age (years) Adapted from Hebert LE, et al. JAMA. 1995;273:1354-1359.
5 65-74 75-84 85+ 4 Number (in millions) 3 of DAT patients in the US 2 1 0 1980 1990 2000 2010 2020 2030 2040 2050
Neuropathological Diagnosis in 233 Community-based Dementia Cases
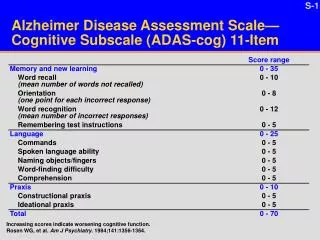
The Office Assessment of AD • A careful history from family member or other informed source. • Quantified assessment of cognitive function--The Mini Mental State Exam (MMSE) • Neurological exam • Laboratory • Repeat assessment in six months
Signs and Symptoms of AD Early Stage Middle Stage Advanced Stage (years 0-4) (years 5-8) (years 8-12) memory loss* memory loss† memory loss‡ executive dysfunction* executive dysfunction† executive dysfunction‡ apathy apathy apathy depression (variable) depression (variable) poor insight poor insight poor insight aphasia* aphasia† aphasia‡ apraxia* apraxia† apraxia‡ disruptive agitation disruptive agitation psychosis psychosis
Motor Symptoms in Parkinson’s Disease • Tremor (resting) • Rigidity • Bradykinesia • Postural instability
Pathology in Parkinson’s Disease • Clinical history of parkinsonism • Neuronal loss and Lewy body inclusions in the substantia nigra, locus coeruleus, basal forebrain and cerebral cortex
Demographic Model for Prevalence of PDD by Duration of PD and Gender 100 80 women 60 Percentage with PDD (%) men 40 20 0 0 2 4 6 8 10 12 14 Duration of PD (years) Dementia in Parkinson’s Disease • Aarsland D et al. Mov Disord. 2005;20:1255-1263. • Robbins JM et al. PARC Working Paper Series. 2001. University of Pennsylvania, Philadelphia.
Cognitive Impairment is Common in Early PD • Norwegian Study • Community sample of incident PD • 196 drug naive PD cases & 201 controls • neuropsych battery • “MCI” = 1.5 SD below norm Aarsland et al, Neurology, 1121-1126, 2009.
Cognitive Impairment is Common in Early PD 19% Aarsland et al, Neurology, 1121-1126, 2009.
Cognitive Impairment is Common in Early PD “These findings highlight cognitive impairment as a key feature from the time of diagnosis of PD” Aarsland et al, Neurology, 1121-1126, 2009.
What is the Pathologic Basis of Dementia in PD?
Clinical Diagnosis of PDD • 2007 Clinical Diagnostic Criteria • Diagnosis of PD • Dementia syndrome within the context of established PD • impairment in more than one cognitive domain • decline from premorbid level • deficits severe enough to impair daily life Emre M, et al. Mov Disord, 22:1689-1707, 2007
Signs and Symptoms of DLB/PDD Early Stage Middle Stage Advanced Stage (years 0-4) (years 5-8) (years 8-12) memory loss* memory loss† memory loss‡ executive dysfunction* executive dysfunction† executive dysfunction‡ apathy apathy apathy depression depression (variable) poor insight poor insight poor insight aphasia* aphasia† aphasia‡ apraxia* apraxia† apraxia‡ psychosis disruptive agitation disruptive agitation
Consensus Criteria for Dementia with Lewy Bodies 1. …progressive cognitive decline of sufficient magnitude to interfere with normal social or occupational function… 2. Core features (2 = “probable”, 1 = “possible”) a. fluctuating cognition, attention, alertness b. recurrent visual hallucinations c. spontaneous features of parkinsonism 3. Suggestive features (plus one core = “probable” DLB) a. REM sleep behavior disorder b. severe neuroleptic sensitivity c. low dopamine transporter uptake (PET/SPECT) 4. One year rule for PDD vs. DLB McKeith et al, Neurology 65:1863-72, 2005.
Signs and Symptoms of DLB/PDD Early Stage Middle Stage Advanced Stage (years 0-4) (years 5-8) (years 8-12) memory loss* memory loss† memory loss‡ executive dysfunction* executive dysfunction† executive dysfunction‡ apathy apathy apathy depression depression (variable) poor insight poor insight poor insight aphasia* aphasia† aphasia‡ apraxia* apraxia† apraxia‡ psychosis disruptive agitation disruptive agitation * mild † moderate ‡ severe
Other Non-Motor Symptoms: Sleep • REM Sleep Behavior Disorder (RBD) • strongly associated with Lewy body pathology • “acting out dreams” • responds to clonazepam, melatonin • Other sleep disturbance • excessive daytime sleepiness • sleep apnea, periodic leg movments, restless leg
Consensus Criteria for Dementia with Lewy Bodies • Criteria good predictor of Lewy body pathology (with or without concomitant AD pathology) - high positive predictive value • Criteria poor predictor of the absence of Lewy body pathology - low negative predictive value
Alzheimer’s Disease and Lewy Bodies
Lewy Body Frequency in Alzheimer’s Disease • Classic Lewy bodies • 21 to 55% • All LRP (including amygdala) • sporadic AD • up to 60% • familial AD • up to 90% Leverenz et al, Arch Neurol, 1986; Ditter et al, Neurology, 1987; Hamilton, Brain Path, 2000, Lippa, Lippa et al, AJP, 1998; Lippa et al Ann Neurol, 1999; Leverenz et al, Arch Neurol, 2006
Cognition in AD, AD/LB, and LB alone DRS MMSE Kraybill et al, Neurology, 2005
LB in FAD (PSEN 1 and 2 mutations) Leverenz et al, Arch Neurol, 2006
Lewy Bodies in AD • LRP is common even in all forms of AD • Pattern of pathological progression distinct • amygdala most vulnerable site • Clinical impact in AD • AP-AD with aggressive course/PDism • Limbic/neocortical with VH • Genetic factors play a role for LRP in FAD
“Pick’s Disease” • 1892 • 71 y.o. man with 3 yr history • Aphasia with paraphasic errors • Difficulty recognizing objects • Autopsy examination with Chiari found prominent frontotemporal atrophy • 1904 • Several additional cases with behavioral and language problems • “Circumscribed atrophy” at autopsy
“Pick’s Disease” • 1911 • Pick case • Swollen neurons (ballooned neurons, BN) • Argyrophilic “kugel” (Pick bodies, PB)
“Frontotemporal Dementia”Current (2008) Proposed Clinical Syndromes • bvFTD • Language syndromes • Semantic • Progressive nonfluent aphasia • Logopenic aphasia • FTD – MND Josephs KA, Ann Neurol, 64:4-14, 2008.
“Frontotemporal Dementia”Current (2008) Proposed Clinical Syndromes • Parkinsonian disorders (4R tauopathy) • Progressive supranuclear palsy • Corticobasal syndrome Josephs KA, Ann Neurol, 64:4-14, 2008.
“Frontotemporal Dementia”Current (2008) Proposed Neuropathologic Types • “15 different pathologies can underlie FTD and related disorders” • Dementia lacking distinctive histopathology • Most TDP-43 positive (FTLD-U • 3R tauopathy • 4R tauopathy • Intermediate filament • No clear distinct inclusion Josephs KA, Ann Neurol, 64:4-14, 2008.
“Frontotemporal Dementia”Core Clinical Features – Behavioral Disorder • Loss of personal and social awareness • neglect of hygiene/grooming, restaurant behavior • Disinhibition • Pseudobulbar palsy, social/sexual, pacing • Mental rigidity/inflexibility • Hyperorality • Stereotyped behavior, pacing, hoarding, toileting • Utilization behavior • Distractibility, impulsivity, impersistence • Loss of insight Lund & Manchester Groups, JNNP, 57:416-8, 1994.
“Frontotemporal Dementia”Core Clinical Features – Behavioral Disorder Mental rigidity/inflexibility Interviewer: What does it mean when people say “Rome wasn’t built in a day”? Patient: “ I’ve been there and I know what they mean!” Interviewer: “Does is have any meaning in our day to day lives?” Patient: “No”
“Frontotemporal Dementia”Core Clinical Features – Affective Disorder • “Depression”, anxiety, sentimentality, suicidal and fixed ideation, delusion • Hypochondriasis, bizarre somatic preoccupation • Emotional indifference (…lack of empathy) • Amimia (inertia, lack of spontaneity) Lund & Manchester Groups, JNNP, 57:416-8, 1994.
“Frontotemporal Dementia”Core Clinical Features – Speech Disorder • Progressive reduction in speech • Stereotypy of speech • Repetition of limited repertoire of words, phrases, or themes (“time to go to lunch?”) • Echolalia and perseveration • Late mutism • All of the aphasic syndromes • expressive (PPA), receptive (semantic), conduction (logopenic) Lund & Manchester Groups, JNNP, 57:416-8, 1994.