Download

1 / 56
930 likes | 3.96k Views
Chronic Otitis Media (COM) with and without Cholesteatoma Pathophysiology, Diagnosis, and Management. Abraham Jacob, MD Otolaryngology – Head and Neck Surgery Otology, Neurotology, and Cranial Base Surgery The Ohio State University.

E N D
Chronic Otitis Media (COM) with and without CholesteatomaPathophysiology, Diagnosis, and Management. Abraham Jacob, MD Otolaryngology – Head and Neck Surgery Otology, Neurotology, and Cranial Base Surgery The Ohio State University Images used in this lecture were obtained from the presenter’s collection, various textbooks and internet websites. Their use is for educational purposes only.
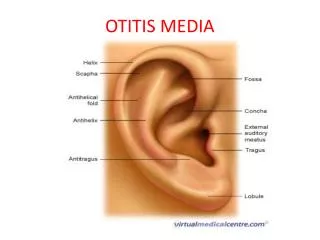
Objectives • To define the normal anatomy and physiology of the ear, Eustachian tube, and lateral skull base. • To understand the role of Eustachian tube dysfunction in the development of chronic ear disease. • To define chronic otitis media (COM) with and without cholesteatoma. • To define the various types of cholesteatoma and how they develop. • To understand the clinical presentation and diagnostic evaluation of COM. • To provide an overview of the surgical management of COM.
The Temporal Bone Made up of the squamous bone, the petrous bone, the tympanic bone, and the styloid process. The mastoid is a part of the petrous bone.
The Eustachian Tube • Connection between middle ear (ME) & nasopharynx (NP) • Medial 2/3 fibro-cartilage; lateral 1/3 bony • Equalizes ME pressure with atmospheric pressure • Allows air into the middle ear and mastoid to spur air cell development • Lined with respiratory epithelium • Mucociliary clearance towards the NP – drains fluid from ME • Usually closed to prevent reflux of NP contents into ME • 13 mm @ birth; 36 mm in adulthood • More horizontal at birth; elongates and descends over time
Eustachian Tube Embryology • ET and middle ear develop from the first pharyngeal pouch (endoderm) • The external ear canal develops from the first branchial cleft (ectoderm) • The ossicles develop from the 1st and 2nd branchial arches • The interface between the first pharyngeal pouch and the first branchial cleft is the tympanic membrane
Eustachian Tube Dysfunction • Abnormal cranial base anatomy • Bony anatomy • Abnormal musculature • Tensor veli palatini and/or levator veli palatini • Inflammation/edema • Physical obstruction • Usually “too closed” but can also be “too open” (patulous Eustachian tube)
Eustachian Tube Dysfunction • ETD is central to the development of otitis media • Acute otitis media • Recurrent acute otitis media (ROM) • Otitis media with effusion (chronic non-suppurative otitis media) • Middle ear atelectasis • Chronic suppurative otitis media • Without cholesteatoma • With cholesteatoma
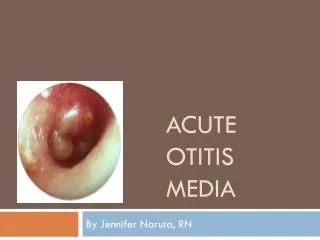
Acute Otitis Media (AOM) • The diagnosis of AOM requires: • History of acute onset signs and symptoms • Presence of middle ear effusion (MEE) • Signs and symptoms of middle ear inflammation • The presence of MEE is indicated by: • A bulging tympanic membrane • Limited or absent tympanic membrane mobility • Air-fluid level behind the TM • - Otorrhea (drainage from the ear) • Signs of middle ear inflammation include: • Erythema of the tympanic membrane • - Otalgia (ear pain)
Etiology of Acute Otitis Media • S. pneumoniae 25% • H. influenzae 20-25% • M. catarrhalis 10-20% • S. pyogenes (gr. A) 2% • S. aureus 1% • No growth up to 35%
Recurrent Acute Otitis Media • Multiple bouts of acute otitis media with complete resolution between episodes • 4 episodes in 6 months or 6 episodes in 1 year is an indication for tympanostomy tube placement
Otitis Media with Effusion(Chronic non-suppurative Otitis Media) • Middle ear filled with serous or mucoid fluid • No purulence • Often present after acute otitis media is treated appropriately with antibiotics • Most will clear within 3 months
Etiology of OME • 50% sterile to culture • Molecular techniques find bacterial products • When culture +, similar to AOM
Medical Treatment of OME • Observation – many European countries wait 6-9 months prior to placement of ear tubes • Antibiotics • Meta-analysis shows beneficial short-term resolution of OME • Unclear long-term impact • Audiogram at 3 months with persistent effusion to determine impact on hearing
Tympanostomy Tubes • In the US, chronic OME >3mos with hearing loss and/or speech delay is an indication for tympanostomy tube placement • Not just there to “drain fluid” • Bypass Eustachian tube to ventilate middle ear
Middle Ear Atelectasis • Lack of middle ear ventilation results in negative pressure within the tympanic cavity • The ear drum retracts onto structures within the middle ear • The result of long standing Eustachian tube dysfunction • The drum loses structural integrity and becomes flaccid • Contact between the drum and the incus or stapes can cause bone erosion at the IS joint • Can sometimes be treated with tympanostomy tubes
Middle Ear Atelectasis • Patient is at risk for cholesteatoma due to skin accumulation within retraction pockets • Drum contact with the incus and/or stapes cause erosion of the incudostapedial (IS) joint • TM is flaccid and non-vibratory – affects hearing • Early atelectasis may be treatable with tympanostomy tubes • Severe atelectasis requires removal of the flaccid ear drum and replacement using cartilage (cartilage tympanoplasty) • This adds rigidity to the drum at the expense of vibratory capacity
Chronic suppurative otitis media with and without cholesteatoma
Chronic suppurative otitis media without cholesteatoma • Chronic infection of the middle ear with a non-healing perforation of the tympanic membrane • Otorrhea (ear drainage) for 6-12 weeks • Middle ear mucosa becomes edematous, polypoid, or ulcerated • The tympanic cavity usually contains granulation tissue • Most common infecting organisms are Pseudomonas aeruginosa, Staphylococcus aureus, Proteus species, Klebsiella pneumoniae, and diphteroids • Annual incidence approximately 40 cases/100,000 population
Chronic suppurative otitis media without cholesteatoma • Patients present with hearing loss and otorrhea • Pain, vertigo, fevers, facial nerve palsy, mental status changes or fetid drainage signify impending intra-temporal or intra-cranial complications
Cholesteatoma • Cholesteatomas are epidermal inclusion cysts of the middle ear and/or mastoid with a squamous epithelial lining • Contain keratin and desquamated epithelium • Term “cholesteatoma” coined by Johannes Muller in 1838 • Misnomer because the cysts don’t contain cholesterol • Can be congenital or acquired • Natural history is progressive growth with erosion of surrounding bone due to pressure effects and osteoclast activation
Cholesteatoma • Annual incidence is unknown • In 1978, there were 4.2 hospital discharges per 100,000 with cholesteatoma (Ruben RJ: The disease in society: evaluation of chronic otitis media in general and cholesteatoma in particular. In Sadé J, editor: Cholesteatoma and mastoid surgery, Amsterdam, 1982, Kugler Publishing) • Harker and coworkers estimated the incidence at 6/100,000 (Harker LA: Cholesteatoma: an incidence study. In McCabe BF, Sadé J, Abramson M, editors: Cholesteatoma: first international conference, Birmingham, Alabama, 1977, Aesculapius Publishing) • Tos and colleagues found 3/100,000 in children and 12.6 per 100,000 in adults (Tos M: Incidence, etiology and pathogenesis of cholesteatoma in children, Ann Otol Rhinol Laryngol 40:110, 1988)
Congenital cholesteatoma • Epidermal inclusion cysts usually present in the anterior superior quadrant of the middle ear near the Eustachian tube orifice • Michaels found epidermoid formation in 37 of 68 temporal bones of fetuses at 10 to 33 weeks' gestation. (Michaels L: An epidermoid formation in the developing middle ear; possible source of cholesteatoma, Otolaryngol 15:169, 1986) • Diagnosed as a pearly white mass behind an intact tympanic membrane in a child who does not have a history of chronic ear disease
Acquired Cholesteatoma Pathogenesis • Invagination • Basal cell hyperplasia • Migration (through a perforation) • Squamous metaplasia
Primary acquired cholesteatoma • Retraction pocket cholesteatoma usually within the pars flaccida or posterior superior tympanic membrane (invagination Theory) • Secondary to ETD • Keratin debris collects within a retraction pocket Mucoid effusion and primary acquired cholesteatoma Mesotympanic cholesteatoma Normal TM
Secondary Acquired Cholesteatoma • Migration Theory – most accepted • Originates from a tympanic membrane perforation • As the edges of the TM try to heal, the squamous epithelium migrates into the middle ear
COM with and without cholesteatomaDiagnosis • History, physical examination, high resolution CT scan of the temporal bone Axial Section Coronal Section
Chronic suppurative otitis media without cholesteatoma • Ototopical antibiotics • Surgical repair of the TM perforation • Repair of the ossicular chain if necessary
Ototopical Medications • Antibiotic only otic drops Floxin (ofloxacin) • Antibiotic with steroid otic drops Ciprodex (ciprofloxin and dexamethasone) Cipro HC (ciprofloxin and hydrocortisone) Cortisporin (neomycin, polymyxin, and hydrocortisone) • Ophthalmic antibiotic preparations Tobradex (tobramycin and dexamethasone) The concentration of antibiotic in ototopical drops is 100-1000x greater than what can be achieved systemically.
Tympanoplasty • Paper patch myringoplasty • Fat myringoplasty • Underlay tympanoplasty (medial graft technique)
Chronic suppurative otitis media with cholesteatoma • Ototopical antibiotics • Surgical repair of the TM perforation • Repair of the ossicular chain if necessary • Often requires mastoidectomy
Mastoidectomy • Intact (bony ear) canal wall mastoidectomy • Canal wall down mastoidectomy • Radical Mastoidectomy • Modified Radical Mastoidectomy
Mastoidectomy Tympanoplasty with mastoidectomy and hydroxyapatite bone cement ossicular reconstruction