Otitis Media
Otitis Media. Mary Bennett, Amanda Buisman & Roline Campbell. Pertinent Anatomy. Ossicles (malleus, incus, stapes). OR Auricle. External Ear Canal. OR Tympanic Membrane. Pertinent Anatomy. (Cone of light). Physiology of the Ear. External Ear


Otitis Media
E N D
Presentation Transcript
Otitis Media Mary Bennett, Amanda Buisman & Roline Campbell
Pertinent Anatomy Ossicles (malleus, incus, stapes) OR Auricle External Ear Canal OR Tympanic Membrane
Pertinent Anatomy (Cone of light)
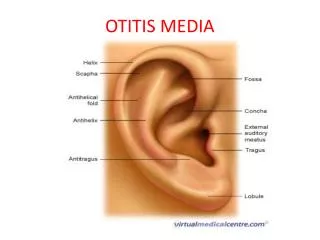
Physiology of the Ear External Ear Consists of the pinna(auricle) and the auditoryearcanal • The pinna functions to both protect the tympanic membrane, and to collect sound waves. • The auditory ear canal distributes sounds in the form of pressure waves to the tympanic membrane.
Physiology of the Ear Middle Ear Consists of the tympanicmembrane, auditoryossicles(malleus, incus, stapes) and the eustachian tube. • The tympanic membrane receives sound waves (in the form of pressure waves) from the auditory ear canal and converts the waves into mechanical vibrations by way of the auditory ossicles. The mechanical vibrations are then transmitted to the inner ear. • The eustachian tube links the pharynx to the middle ear and while it is normally closed, it can let a small amount of air though to equalize the pressure between the middle ear and the atmosphere. It also drains mucous from the middle ear.
Physiology of the Ear Inner Ear Consists of the semicircular canals, vestibule, acoustic nerve, and the cochlea. • Mechanical vibrations are received from the TM and are transformed into fluid vibrations, which are then converted into nerve impulses by nerve endings located in the cochlea. These impulses are conducted via the auditory nerve to higher levels and interpreted as sound by the brain. • The semicircular canals and vestibule function to maintain balance and equilibrium.
Pathophysiology of Otitis Media (OM) OM is defined as inflammation in the middle ear without reference to etiology. OM is one of the most common reasons for a child to visit the pediatrician. OM can be classified into four categories; • Acute Otitis Media (AOM) • Otitis Media with Effusion (OME) • Recurrent AOM • Chronic OME
Pathophysiology of Acute Otitis Media (AOM) The most important factor in the pathogenesis of AOM is abnormal function of the eustachian tube. • Reflux, aspiration, or insufflation of nasopharyngeal bacteria into the middle ear via the dysfunctional eustachian tube may lead to infection. • Eustachian tube dysfunction occurs due to either abnormal patency, or obstruction (either functional or mechanical).
Pathophysiology of Acute Otitis Media (AOM) Common causative microorganisms for AOM are: • Streptococcus pnumoniae (30-50% of cases) • Haemophilus influenzae (20-30% of cases) • Moraxella catarrhalis (7-25% of cases)
Acute Otitis Media (AOM)With and Without Perforation When AOM is present and the TM is intact, it is referred to as “AOM without perforation”. When AOM is present and the TM is NOT intact, it is referred to as “AOM with perforation”.
AOM with Perforation AOM with perforation has two categories; • AOM complicated by perforation of the tympanic membrane presenting as otorrhea. (Left) • AOM in a patient with tympanostomy tubes. (Right)
OM with Effusion (OME) OME occurs when thick fluid accumulates behind the TM. OME typically occurs immediately following treatment of AOM due to the resolution of acute inflammation, allowing visualization of the middle ear fluid behind the TM.
Epidemiology The overall prevalence of AOM is 15-20%, with the highest peak at 6-36 months of age. An additional smaller peak occurs at 4-6 years of age. Between 60-80% of infants have had at least one episode of AOM by one year of age. AOM is uncommon in older children and adolescents.
Epidemiology AOM is more common in boys, and the prevalence is greatest in Alaskan natives and Native Americans (Caucasian race is also considered a risk factor however). AOM is most common in the winter months and in early spring, coinciding with peaks in the incidence of URI’s.
Epidemiology Risk factors for developing OM; • Male gender • Absence of breastfeeding • White race • Passive exposure to tobacco smoke • Daycare attendance • Low socioeconomic status • Presence of siblings in the household • Altered host defenses/underlying conditions
Patient Evaluation-History Clinical presentation- children with AOM often have a history of rapid onset of fever and ear pain (usually within 48 hours). The patient may also have hearing loss, otorrhea, and irritability. Nonverbal children present with “ear pulling” and generalized fussiness. Associated symptoms include URI, cough, diarrhea, and nonspecific complaints such as decreased appetite, waking at night, or irritability in infants.
Patient Evaluation- History It is important in the history to differentiate nonspecific symptoms of OM from those indicating a more serious condition such as meningitis. For infants or children with a history of persistent or recurrent OM, it is important to find out when they had their last documented infection and what treatment they received.
Patient Evaluation- History Helpful questions to ask when obtaining the patient’s history; • Does the infant have fever, ear pain, hearing loss, or otorrhea? • Is the infant/child inconsolable or lethargic? • Has the infant/child had a previous ear infection? If so, when? • Did the child complete the course of prescribed antibiotics?
Helpful Questions • How many ear infections has the child had in the past year? • Is the child taking any medication to prevent recurrent OM? • Does the child attend daycare? • Is the child exposed to passive smoke? • Is the infant breast-fed? • Does the child appear to hear? • Is the child’s speech development normal?
Physical Exam Findings To diagnose OM, the TM must be visualized. The position, color, degree of translucency, and mobility of the TM must be evaluated. Classically, in AOM the TM is full or bulging, opaque, and has limited or no mobility, or is retracted. The light reflex is usually absent or distorted.
Physical Exam Findings Associated physical exam findings may include; • posterior auricular and/or cervical adenopathy • pain on movement of the pinna • anterior ear displacement *The presence of these symptoms may also suggest a more serious condition such as mastoiditis therefore thorough history taking and visualization of the TM is essential.
Normal (no AOM present) Exam Findings Position- process of the malleus should be visible but not prominent through the membrane. Color- pearly gray. Translucency- middle ear or bony landmarks should be visible through the TM. Mobility- normal ear will move with pneumatic otoscopy.
Physical Exam Findings Here is a normal TM
Physical Exam Findings Here is a picture of a typical TM with AOM. The TM is noted to appear erythematous or injected in color, the light reflex is absent, landmarks are poorly visualized, and there is a poor degree of translucency.
Physical Exam Findings Here is an example of AOM with a bulging TM. Note the color, position, transparency, lack of visible landmarks, and distorted light reflex
Physical Exam Findings Here is a retracted TM
Diagnosis of AOM • Accuracy in diagnosis of utmost importance • Ensures appropriate treatment for AOM • Avoids unnecessary use of antibiotics in OME • Prevents overuse of antibiotics – considered a major factor in increased drug-resistance
AOM in Infants & Children • Challenges in establishing a diagnosis: • Uncooperative • TM obscured by cerumen • Symptoms of AOM may overlap with other conditions (URI) • Symptoms may be subtle or even absent • Successful diagnosis facilitated by: • Systematic assessment • Stringent diagnostic criteria • Training and experience
AAP & AAFP Diagnostic Criteria Three diagnostic criteria 1. Recent, abrupt onset of ME inflammation & effusion (ear pain, irritability, otorrhea, and/or fever) 2. MEE confirmed by: • bulging TM, • limited or absent mobility (pneumatic otoscopy), • air-fluid level behind TM, or • Otorrhea (with TM not intact) 3. Evidence of ME inflammation - confirmed by: • distinct erythema of TM, or • distinct otalgia interfering with normal sleep or activity
Diagnostic Techniques • Pneumatic otoscopy • Assess inflammation • Assess effusion • Assess perforation & character of otorrhea • Tympanometry and/or acoustic reflectometry • Assess/confirm effusion • Tympanocentesis (by otolaryngologist) • Identify infectious organism • Use in special populations
Accurate & objective assessment of effusion • Requires an air-tight seal & pressurization of the ear canal • Painful & uncomfortable for children • Limited use & costly Tympanometry Acoustic Reflectometry Analyzes sound reflected off the TM to detect MEE No pressure seal required Small quantity of cerumen does not affect this test Increased use in primary care
Pneumatic Otoscopy • Allows direct visualization of TM & ear structures to confirm presence of inflammation, effusion and assess for perforation. • Important to: • Remove cerumen obscuring TM • Ensure adequate lighting • Appropriately restrain the child to allow examination & prevent injury • For pneumatic otoscopy – adequate airtight seal by choosing correct size and shape speculum.
Assessment of the TM • Locate border between external ear canal & TM • Assess: • Surface • Opacity • Color • Mobility • Other findings
The Surface of the TM • Are the landmarks visible? • Are the landmarks obscured or unusually prominent? • Where is the cone of light? • Is the TM intact?
Retracted & Bulging TM Abnormally retracted TM Bulging TM
Opacity of the TM Normal Tympanic Membrane - Usually translucent • Scarred Tympanic Membrane • note loss of translucency • at area of scar
Color of the TM Expected Findings AOM with infused erythema • Normal TM = Pearly grey • Crying infant = Pink TM • Classic AOM = red or infused TM • Atypical AOM = white or yellow TM (from purulent middle ear fluid)
Mobility of the TM • Successful pneumatic otoscopy requires airtight seal of external ear canal • With normal mobility the TM will • move inward when positive pressure is applied • move outward when negative pressure is applied • A retracted TM will show • decreased or absent inward deflection • but normal outward deflection with negative pressure • Crying children have increased middle ear pressures during exhalation which fleetingly normalize during inspiration • Severely diminished or absent mobility is indicative of effusion
Other Findings Cholesteatoma → ↖ Bleb / blister Air-fluid level behind the TM - Indicative of Middle Ear Effusion (MEE) Cholesteatoma – grey or white mass behind the TM Blebs / blisters on the surface of the TM – Bullous Myringitis
Clinical Diagnosis of AOM Requires: Acute onset of symptoms AND Middle Ear Effusion AND Middle Ear Inflammation OR Acute purulent otorrhea via perforated TM or tympanostomy tube AND otitis externa has been excluded
Differential Diagnoses Diff. Dx S & S
AOM or OME? Two year old Ron’s mom reports him rubbing and slapping at his left ear since early this morning. He refused breakfast and has been irritable all day. Pneumatic otoscopy reveals a bulging, yellow tympanic membrane with marked decrease in mobility. Is this AOM or OME?
Summary: MEE • MEE (Middle Ear Effusion) = fluid in middle ear • Occurs in both AOM and OME • OME often precedes development of AOM • OME mostly also follows resolution of AOM
OM with ruptured TM AOM with TM intact AOM with ruptured TM (or with Tympanostomy tube) History of acute onset otalgia which improved when ear started draining (relief of pressure when TM ruptured) Inflamed TM TM ruptured & draining purulent fluid into external ear canal • Acute onset otalgia • Inflamed TM • Middle Ear Effusion present (Bulging and decreased mobility)
Treatment of AOM • Clinical course of 24 – 72 hours with appropriate antimicrobial Rx • Slightly slower resolve of acute symptoms when not treated • MEE may persist for weeks or months
Clinical Practice Guideline • AAP and AAFP Clinical Practice Guidelines (2004) state that the following aspects of management should be considered: 1. Symptomatic therapy 2. Observation (“Watchful waiting”) 3. Appropriate antimicrobial therapy
1. Symptomatic Therapy - Pain • Acetaminophen • 10 -15mg/kg PO/PR every 4 – 6 hours as needed • not to exceed 90mg/kg/day • Ibuprofen • 5 - 10mg/kg PO/PR every 6 – 8 hours as needed • not to exceed 40mg/kg/day • Topical agents • Antipyrine-benzocaineotic drops • 4 – 5 drops into affected ear(s) every 2 hours as needed • not to be given in case of TM perforation • Aqueous lidocaine ear drops (30 minute efficacy – needs further evaluation – not currently a recommendation)
Treatment of pain (cont.) • Complementary treatments • Herbal extracts: • OtikonOtic solution • Compared well to topical anesthetic • Home remedies • Distraction • External application of heat or cold • Instillation of oil into external auditory canal • Clinical evidence still lacking