Download
1 / 102
1.08k likes | 2.41k Views
Dysphagia and Dysphonia following Organ Preservation for Head & Neck Cancer Treatment. ASHA Convention Boston, 2007 Donna Tippett, Heather Starmer, Kim Webster Johns Hopkins University Department of Otolaryngology, Head & Neck Surgery. Outline. Introduction to organ preservation

E N D
Dysphagia and Dysphonia following Organ Preservation for Head & Neck Cancer Treatment ASHA Convention Boston, 2007 Donna Tippett, Heather Starmer, Kim Webster Johns Hopkins University Department of Otolaryngology, Head & Neck Surgery
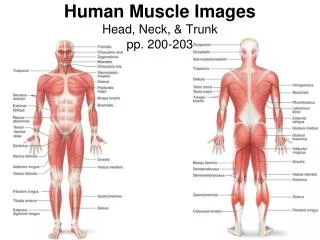
Outline • Introduction to organ preservation • Oral motor exercises and dysphagia • Related toxicities • Trismus • Xerostomia • Dysphonia • Quality of Life • Summary, questions & answers
Learner objectives • Demonstrate understanding of functional impact of organ preservation approaches on swallowing and voice • Discuss the impact of toxicities on swallowing and voice • Describe therapeutic interventions that may be beneficial • Discuss current literature influencing clinical decision making
Terminology • Organ preservation • Organ conservation • Primary radiotherapy • Chemoradiation • Induction chemotherapy • Adjuvant chemo-/radiotherapy • Neoadjuvant • Combined modality • Clinical trials and protocols
Functional Outcomes and H&N Cancer • Treatment modality • Locus of tumor • Other factors
Age Gender Culture Family support Previous swallowing problems Motivation Geographic location Other health history Occupation Complications Prioritizing Quality of life Patient Factors
Sticking Pain No appetite Trismus Nausea Vomitting Dry throat Fear Mucositis No taste or smell Choking Dry mouth Swelling Fistula No energy Fatigue Stitches
Tracheostomy tubes: Can reduce laryngeal elevation Irritation of airway Can reduce laryngeal sensation Occlude for swallow Window Feeding tubes: Reduce anxiety Allows for learning Greater energy Maximize nutrition Other Considerations
Mucositis Xerostomia Edema Trismus Dental caries Candida Altered smell and taste Reduced appetite Fibrosis Osteoradionecrosis Odynophagia Predicting Dysphagia from TxRADIATION THERAPY may cause:
Swallowing post XRT Oropharyngeal Symptoms • Reduced soft palate elevation • Reduced swallow initiation • Reduced BOT retraction • Thickened immobile epiglottis • Reduced laryngeal elevation • Reduced airway protection • Reduced pharyngeal contraction • Reduced cricopharyngeal opening • Stricture(s) • Webs
Predicting Dysphagia from Tx Chemotherapy/Organ Preservation: • Nausea • Oral mucositis • Fatigue • Other side effects from radiation ’d • Longer recovery from effects Preservation of organ ≠ preserved function
Fibrosis Xerostomia Edema Mucositis Atrophy Decreased pliability of the vocal folds Reduced glottic closure Impaired vibration of the mucosal surface Reduced amplitude of vibratory excursion Supraglottic compensation Predicting Dysphonia from TxRADIATION THERAPY may cause:
Voice post XRT Voice symptoms: • Reduced pitch variability • Reduced loudness • Reduced phrase length • Hoarse or breathy vocal quality • Vocal strain • Vocal fatigue • Reduced ability to sing
Dysphagia Treatment at JH • Before organ preservation therapy • Educate • Exercise • Evaluate • During • Make behavioral accommodations, modifications • Review exercises, should be done daily if possible • Monitor/Evaluate • After • Evaluate; changes occur up to 15 years later • Continue home exercises for a minimum of 4-6 weeks after tx • Initiate formal dysphagia tx as indicated
Dysphonia Treatment at JH • Before organ preservation therapy • Educate • Exercise • Evaluate • During • Make behavioral accommodations, modifications • Review exercises, should be done daily if possible • Monitor/Evaluate • After • Evaluate as needed • Continue prophylactic exercises for at least 4-6 weeks after tx • Implement formal intervention if necessary
Pre-treatment Information • Reduces anxiety • Improves post-treatment compliance • Involves the patient as a team member • Better post-tx speech targets • Assess writing, legibility, socio- and occupational communication needs Lazarus, 2005; Glaze, L. 2005
Medical/Surgical Tx for Dysphagia/Dysphonia • Vocal fold medialization by injection • Dilatation • Surgery • Cricopharyngeal myotomy/Botox • Soft tissue augmentation (tongue base) • Oral prosthetics • Supraglottic/glottic closure • Medialization thyroplasy • Laryngotracheal separation (LTS) • Total laryngectomy • Rerouting salivary ducts • Dennervation of salivary glands
Organ Preservation Approachesand Dysphagia • Nature of dysphagia after organ preservation tx • Recovery of swallowing function • Swallowing intervention
Characteristics of Dysphagia • Goguen et al, 2006 • Prospective cohort study • N = 23 s/p CRT for head/neck SCCA • Common deficits • Decreased epiglottic tilt • Decreased BOT retraction • Decreased laryngeal elevation • Impaired bolus propulsion • Laryngeal penetration/aspiration • 14/23 pharyngoesophageal narrowing
Characteristics of Dysphagia • Dworkin et al, Dysphagia, 2006 • Retrospective study • Performed FEES in individuals with Stage III/IV laryngeal SCCA • Multiple decompensations • Excess oropharyngeal secretions • Premature spillage into vallecula • Retention in vallecula • Post cricoid residue • Laryngeal penetration/aspiration
Characteristics of Dysphagia • Logemann et al, Head Neck, 2006 • Examined differences in swallowing across tumor sites and CRT protocols • VFSS pre- and 3 months post tx • N = 53 with Stage III/IV head/neck SCCA • Common deficits • Reduced BOT retraction • Reduced tongue strength • Delayed laryngeal vestibule closure
Characteristics of Dysphagia • Pauloski et al, Head & Neck, 2006 • Prospective cohort study • VFSS pre- and post tx • N = 170 with head/neck SCCA • Identified multiple decompensations • Limitations in oral intake and diet post tx were significantly related to: • Reduced laryngeal elevation • Reduced CP opening • Rating of nonfunctional swallow on at least 1 bolus type
Recovery • Goguen et al, Otolaryngol Head Neck Surg, 2006 • Prospective cohort study • F/u at 3, 6, 9, 12, 24 months post tx • N = 59 • Primary tumor sites: oral cavity, oropharynx, hypopharynx, larynx
Recovery • Goguen et al, 2006
Recovery • Dworkin et al, Dysphagia, 2006 • N = 14 with Stage III/IV laryngeal SCCA • <12 months: 43% regular/near normal diet • >12 months: 86% regular/near normal diet
Recovery • Pauloski et al, 2006
Dysphagia Therapy • Targets • BOT retraction • Tongue strength • Laryngeal elevation Goguen et al, 2006 Logemann et al, 2006 Pauloski et al, 2006
EBP • Internal source of information • Best clinical judgment • Knowledge of anatomy/physiology • External source of information • Electronic database search • PubMed Clinical Queries Coyle J & Leslie P, Perspectives on Swallowing and Swallowing Disorders, 2006
Exercise Principles • Goal selection • Specificity of training • Overload/progression Clark H, AJSLP, 2003
Exercise Principles • Goal selection • Specificity of training • Overload/progression Clark H, AJSLP , 2003
Exercise Principles • Goal selection • Specificity of training • Overload/progression Clark H, AJSLP , 2003
Theoretically Sound Exercise • Mendelsohn maneuver • Addresses goals for: • Stretching: maintaining maximum laryngeal elevation over several seconds • Strengthening: sustaining laryngeal elevation against resistance • Meets criteria for specificity and progression Clark H, AJSLP , 2003
Theoretically Sound? • Tongue resistance exercise • Involves an isometric, static contraction • Address strengthening • May meet the criteria for progression • Does not meet criteria for specificity
Swallowing Maneuvers Supraglottic, super-supraglottic, tongue-hold, effortful swallow, and Mendelsohn Increased laryngeal elevation and laryngeal vestibule closure with maneuvers Improved airway protection Tongue base-pharyngeal wall pressures and contact duration increased with maneuvers Lazarus et al, Head Neck,1994 Logemann et al, Head Neck, 1997 Lazarus et al, Folia Phoniatri Logopaed, 2002
Theoretically Sound? • Voluntary swallow maneuvers • May address strengthening and/or stretching • May meet the criterion for progression • Meet the criterion for specificity
Swallowing Intervention • Kulbersh et al, Laryngoscope, 2006 • Cross sectional analysis of QOL to determine efficacy of pre-tx intervention • Administered MDADI • N = 25 pre tx swallowing exercises • N = 12 post tx swallowing exercises
Swallowing Intervention • Kulbersh et al, 2006 • Adjusted Mean Scores on MDADI
Efficacious Approach • Need to determine what you are targeting • Specify the rationale for tx • Match the exercise as closely as possible to the desired outcome • Try exercises at baseline • Document changes in fx, QOL, weight
Trismus • Dijkstra et al , Oral Oncol, 2004 • Prevalence 5% - 38% in head/neck cancer • Variation secondary to lack of uniform criteria, visual assessment, retrospective review
Criteria for Trismus • Normal MIO 46+7mm Steelman et al, Mo Dent J, 1986 • MIO < 30 – 35mm Buchbinder et al, J Oral Maxillofac Surg, 1993; Dijkstra et al, J Oral Maxillofac Surg, 2006
Treatment for Trismus • Buchbinder et al, J Oral Maxillofac Surg, 1993 • N = 21 s/p resection of oral SCCA and radiation tx <5 years
Treatment for Trismus • Cohen et al, Arch Phys Med Rehab, 2005 • N = 7 s/p surgery for oropharyngeal SCCA p < .01
Treatment for Trismus • Dijkstra et al, Oral Oncology, 2007 • Retrospective study • N = 27 patients with trismus secondary to head/neck SCCA and 8 with trismus secondary to other dx • Treatment included • Active ROM • Hold relax techniques • Manual stretching • Joint distraction • Use of devices and tools
Treatment for Trismus • Dijkstra et al, 2007 p < .05
Oral Health • Xerostomia • Relationship between oral hygiene and aspiration • Oral cancer self-examination
XerostomiaVisual Inspection of the Mouth • Tongue depressor sticks to buccal mucosa • “Lipstick” sign • Dry, sticky or erythematous oral mucosa • Red patches on palate, tongue • Decreased lingual papillae • Little pooled saliva in FOM • Stringy, ropy, foamy saliva