
Vesiculobullous disease
E N D
Presentation Transcript
1. Vesiculobullous disease
9. Pemphigus groups
10. Classification Pemphigus vulgaris :
Pemphigus vegetans : Localized
Drug-induced
Pemphigus foliaceus
Pemphigus erythematosus : Localized
Fogo selvagem : Endemic
Drug-induced
11. Classification Paraneoplastic pemphigus
IgA pemphigus :
Sub-corneal pustular dermatosis
Intraepidermal neutrophilic IgA dermatosis
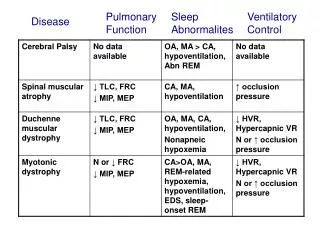
12. Pemphigus Two major types: Vulgaris and foliaceus.
Pemphigus vulgaris: Erosions on mucous membranes and skin; flaccid blisters on skin
Pemphigus foliaceus: Crusted, scaly skin lesions
Pathology.
Pemphigus vulgaris: Suprabasilar acantholysis
Pemphigus foliaceus: Sub-corneal acantholysis
13. Causes Common causes :
Pemphigus is an autoimmune disease
Caused by autoantibodies against keratinocyte proteins desmoglein-1 and desmoglein-3
15. Causes Rare causes :
Penicillamine: 9% of rheumatoid arthritis patients develop pemphigus
Captopril, rifampin, and meprobromate have been associated with pemphigus
16. Contributory or predisposing factors Pemphigus can occur in association with myasthenia gravis
Certain human leukocyte antigen (HLA) types predispose: HLA DR4, DR6, and A10
17. Age
40-60 years
Rare in children
Gender
Occurs in equal numbers in men and women.
Race
More common in Ashkenazi Jews and in people of Mediterranean decent.
Genetics
Associated with HLA DR4, DR6, and A10.
18. Symptom Painful blisters in the mouth appear first, and may lead to weight loss
Blisters occur on the skin and mucosal areas, especially where trauma and pressure applied
Large areas of affected skin seep and crustation
Fever and malaise
Pruritus normally absent
19. Signs Skin or mucosae can just shear off leaving widespread painful erosions
Nikolsky's sign - epidermis is easily detached from underlying skin
20. Flaccid bullae of various sizes
Bullae arise from 'healthy' skin, rupture, and leave crusting and denuded skin
Any area of stratified epithelium can be affected
21. Signs Lesions often appear first in the mouth prior to skin involvement
Extent of skin and mucosal involvement varies
Eyes, nasal mucosa, and genitalia may be affected
Lesions may occur in oropharynx and upper esophagus
Pyrexia and systemic features common
Secondary infection is common
22. Skin biopsy Acantholysis and intraepidermal separation of keratinocytes, is likely to have pemphigus vulgaris.
Diagnosis is confirmed by direct or indirect immunofluorescence.
26. Don't miss! Pemphigus vulgaris should be suspected in any bullous or chronic mucosal ulceration
Widespread skin involvement with erosions and bullae requires urgent hospitalization and systemic treatment as morbidity and mortality are high
27. Don't miss! Severe oral ulceration spreading past the vermilion border should raise suspicion of paraneoplastic pemphigus
28. Tzanck test Acantholytic cells
Cause of abnormal result
Pemphigus vulgaris
Other bullous skin diseases
29. Skin biopsy Intraepidermal separation of keratinocytes, forming a split between lower and upper portions of epidermis
Acantholysis - separation of individual epidermal cells from surrounding cells
Mild or absent inflammatory infiltrate
30. DIF Direct immunofluorescence shows immunoglobulin G (IgG) on the keratinocyte cell surface of the patient's skin
Direct detection of tissue-bound antikeratinocyte (desmoglein) antibodies on perilesional skin of the patient
Antihuman IgG and C3 binding detected at epidermal cell surfaces; no deposition along basement membrane
32. IIF Indirect immunofluorescence shows IgG in patient's serum that binds the cell surface of normal keratinocytes.
Autoantigens are desmogleins (transmembrane desmosomal adhesion molecules)
35. Cause of abnormal result
Pemphigus vulgaris.
Other pemphigus variants can yield a positive test
36. Treatment
37. Goals Prevent new lesions forming
Prevent scarring
Prevent secondary infections
Minimize effects of disease on patient's lifestyle
38. Immediate action Patients with widespread disease should be referred for hospitalization and immediate treatment, as morbidity and mortality are high
If secondary skin infection is suspected, immediate antimicrobial treatment should be commenced
Fluid and electrolyte normalization should be achieved
39. Aim of treatment is to prevent eruption of new lesions
40. Specific therapy depends on the extent and severity of the disease
Corticosteroids: topical steroids such as triamcinolone, clobetasol propionate, and fluticasone propionate can be used in mild disease
But most patients require systemic steroids, which have adverse effects
41. Nonalkylating agents (e.g. azathioprine, mycophenolic acid, cyclosporine) are steroid-sparing agents
42. Alkylating agents (e.g. cyclophosphamide, chlorambucil) are steroid-sparing agents
Antibiotics (e.g. tetracycline) have been used in pemphigus, usually in combination with other agents
43. Local antiseptics and analgesics can give symptomatic relief
Anti-inflammatory drugs, such as gold or dapsone, are disease-modifying drugs for severe cases of pemphigus vulgaris
44. Other therapies include plasmapheresis, an inpatient procedure performed by a specialist.
It is used only for refractory cases and results are variable
46. Coexisting disease Thymoma, carcinoma,Myasthenia gravis
The presence of lymphoproliferative disorder should heighten suspicion of paraneoplastic pemphigus
47. Coexisting medication Certain medications can cause pemphigus and should be stopped immediately; most likely is penicillamine for rheumatoid arthritis
Most patients with drug-induced pemphigus go into remission after they stop taking the offending medication
52. Bullous pemphigoid
54. Pathology
60. Treatment Topical steroid
Systemic steroid
Methotrexate
Azathioprine
Cyclophosphamide
Dapsone
IVIG
Plasmapheresis