Download
1 / 50
560 likes | 1.62k Views
Knee Arthroplasty. Degeneration of Knee. Degeneration of Knee (cont’d). Osteoarthritis is the most common cause Abnormalities of knee joint function resulting from Fractures Torn cartilages Torn ligaments can lead to degeneration many years after the injury. Total Knee Arthroplasty.

E N D
Degeneration of Knee (cont’d) • Osteoarthritis is the most common cause • Abnormalities of knee joint function resulting from • Fractures • Torn cartilages • Torn ligaments can lead to degeneration many years after the injury
Total Knee Arthroplasty • Indications for surgery • Pain and disability at the point • When ADL (standing, walking, and climbing stairs) cannot be done • It is an artificial joint • Resurfacing of cartilage and underlying bone • A metal and plastic implant • Corrects deformity
Objectives of TKA • Function • Stability • Motion • Long-term fixation of implants • Correction of deformity • reduce wear
History of TKA • 1863-1921 • Interposition of joint capsule (Verneuil) • Muscle (Ollier) • Fat and fascia (Murphy) • Pig bladder (Campbell) • 1951-1958 • Acrylic hinge (Walldius) • Vitallium femoral hemiarthroplasty (Campbell) • Acrylic two-part prosthesis, first TKA (Judet) • Metallic tibial hemiarthroplasty (Townley) • Metallic hinge (Shiers) • Tibial unicompartmental designs (McKeever and MacIntosh) • 1969 Polycentric TKA (Gunston) • 1970 Bicruciate sacrificing arthroplasty (Freeman and Swanson) • 1971 Improved, refined hinge (Guepar)
History of TKA • 1972-1974 • Polyethylene metal bicondylar anatomic TKA (Townley) • Congruent geometric design (Coventry) • Unicondylar, unicompartmental arthroplasty (Boston and Brigham) • Total Condylar cruciate sacrificing tricompartmental TKA (Insall and Ranawat) • 1975-1978 • Bicruciate retaining metal- backed tibial TKA (Cloutier) • Varus-valgus/ anteroposterior constraint TKA (Walker) • Posterior stabilized TKA (Insall and Burstein) • 1980’s • Low Contact Stress, ACL sparing
Developments in TKA Design • Early designs failed • Loosening, wear, osteolysis, stiffness, dislocation, instability, and extensor mechanism dysfunction • In 1970’s • ~ 300 TKA designs • To provide rotation • Mobile-bearing implants in the 80’s • To reduce wear • Poly concave design
Poly design • Congruent femorotibial articulation • A larger area of contact • Reduces contact stresses High contact Stresses for “Curved-on-Flat” design LCS low contact stress distributed over a large area of polyethylene
Poly design (cont’d) • Sphericity leads to congruency in coronal and sagittal plane • Reducing this mode of wear • Mobility of tibial bearing reduces • Rotational torque • Subsequent loosening of tibial component
Design criteria • Material compatibility and wear • Adequate mechanical strength • Minimization of joint reaction forces • Minimization of fixation interface shear • Avoidance of fixation interface tension\
Design criteria (cont’d) • Uniformity of interface compression • Duplication of anatomical function • Adequate fit for patient population • Manufacturability • Reasonable inventory costs
Implant Wear • Level and type of stresses • On articulating surfaces • Material properties • Imperfections of UHMWPE • Coefficient of friction UHMWPE - ultra-high molecular weight polyethylene
Stresses on Implants • Load • Peak tibiofemoral force during sport activities • Around 7 times the body weight • Contact stresses on UHMWPE • ~ 3 times yield point
Stresses on Implants (cont’d) • Plastic strain of multiple cycles • Material fatigue • Pits, cracks, and delamination • Flake-like wear particles in surrounding tissue Wear particle Polyethylene failure
Material properties • UHMWPE fails first • Wear resistance • Ultimate tensile strength and ductility • Inversely proportional • Increase in ultimate tensile strength • Reduction in toughness • Increase wear rates • Balance the two to increase wear resistance
Material properties (cont’d) • Wear, crack nucleation, occurs due to • Fusion defects • Voids • Quality of resins • Manufacturing processes • Cyclic plastic deformation
Coefficient of Friction • Coefficient of friction depends on • Material • Surface finish of articulating surfaces • Lubricating regimen • Surface roughness can increase in vivo • Entrapment of third body particles • Bone or bone cement • Amount of wear particles can be reduced • If full-fluid lubrication is used
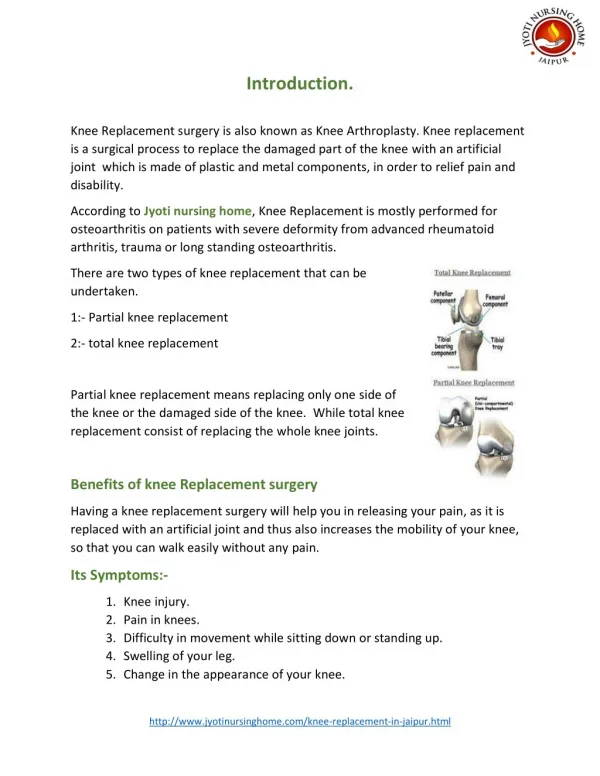
Knee joint components • Knee joint implants consist of • Femoral • Tibial • Patellar component
Femoral Component • Made of a strong polished metal • Cobalt chrome • Radius • Single • Reduced
Femoral Component (cont’d) • Single radius design has same femoral radius from extension to full flexion • Reduced radius design has larger radius near extension and smaller radius at flexion
Tibial Component • Proximal tibia is covered with a metal tray • Tibial component is topped with • Disk-shaped polyethylene insert • May be fixed • Rotates about a stem in rotating platform
Patellar Component • Replaces knee cap
Types of TKA • Condylar TKA • Constrained • PCL sacrificed • Non-Constrained • Mobile TKA • May spare the ACL • Uni • Hinged
Advantages of Mobile TKA • Many components of mobile-bearing knee are same as traditional fixed knee implants • Same proven surgical procedures can be used • Currently used preoperative and postoperative routines for patient are also same
Disadvantages of TKA • Particles polyethylene wear • Lead to aseptic looseningand osteolysis • Destroys a tibial inlay in <10 years • Unexplained pain • Infection • Reduced flexion
Surgical Procedure • An incision is made over the front of the knee and tibia • Femoral condyles are exposed • Bone cuts are made to fit the femoral component
Femoral IM Canal • A reamer is passed through a hole near the center of joint surface of lower end of femur and into femur shaft
Cutting the Distal Femur • A resection guide is attached to lower end of the femur • 8-10 mm Osteo-cartilage surface is removed
Cutting the Distal Femur (cont’d) • Another resection guide is anchored to end of femur • Pieces of femur are cut off the front and back • As directed by the miter slots in guide • Then cuts are made to bevel the end of femur to fit implant
Placing the Femoral Component • Metal component is held in place by friction • In the cemented variety • An epoxy cement is used
Cutting the Tibial Bone • A resection guide is attached to front of tibia • Direction of the saw cuts in 3D • AP tilt • LM tilt • Upper end of tibia is resected
Placing the Tibial Component • Metal tray that will hold plastic spacer is attached to the top of the tibia
Placing the Plastic spacer • Attached to the metal tray of tibial component
Preparing the Patella • The undersurface of the patella is removed
Placing the Patella Component • The patella button is usually cemented into place behind the patella
Animation for TKA • http://www.hipandkneesurgery.net/knee.html
Unicompartmental KA • Unlike total knee surgery this is • Less invasive procedure • Replaces only damaged or arthritic parts i.e. in either compartments
Advantages of Uni • Preservation of the ACL • Smaller incision • Less blood loss • Lower morbidity • Shorter recovery time • Lesser bone removed
Disadvantages of Uni • Inferior survivorship • Error in proper placement of components • Loosening • Prosthetic wear • Secondary degeneration of opposite compartment
Animation for Unicompartmental KA • http://www.hipandkneesurgery.net/repicci.html
Modifications in TKA Design • The New Jersey LCS Knee allows • Bicruciate or posterior cruciate ligament (PCL) retention • Using gliding meniscal bearings or cruciate substitution with rotating platform design • Also provides • Uni mobile-bearing • Mobile- bearing stemmed design
References • http://www.orthobluejournal.com/supp/0202/sorrells/ • http://www.orthobluejournal.com/supp/0202/crossett/Default.asp • http://www.orthobluejournal.com/supp/0202/kuster/