Download
1 / 42
511 likes | 1.08k Views
INFECTION AND TOTAL KNEE ARTHROPLASTY : DIAGNOSIS AND TREATMENT. Scott M. Heithoff D.O. INTRODUCTION . Deep infection is one of the most disastrous complications following total joint arthroplasty The incidence of infection is generally considered to be between 1-2 %

E N D
INFECTION AND TOTAL KNEE ARTHROPLASTY : DIAGNOSIS AND TREATMENT Scott M. Heithoff D.O.
INTRODUCTION • Deep infection is one of the most disastrous complications following total joint arthroplasty • The incidence of infection is generally considered to be between 1-2 % • Rand et al reported on 3,000 TKA’s at the Mayo Clinic with an incidence of 1.2% • Wilson et al reported on 4,171 TKA’s at Brigham and Women’s Hospital with an incidence of 1.6%
RISK FACTORS FOR INFECTION • The risk of acquiring an infection of a TKA can be broken into factors related to the patient and to the surgeon • Host Factors : Usually unable to be altered • Perioperative Factors • Intraoperative Factors • Surgical Technique Factors
RISK FACTORS FOR INFECTION • Host Factors Relative Risk • Rheumatoid Arthritis 3 - 4.4% • Psoriasis 17% • Diabetes 7% • Transplant 14% • Prior Knee Surgery 1 – 4.5%
RISK FACTORS FOR INFECTION • Intraoperative Factors • Operating Room Time • Air Turnover Rate • Laminar Flow • Operating Room Traffic • Body Exhaust Suits
RISK FACTORS FOR INFECTION • Surgical Technique Factors • Hinged Implant • Prophylactic Antibiotics • Iodophor Drape • Previous Incisions • Hematoma • Wound Dehiscence
Most deep infections are caused by Staph Aureus (58 – 63%) Two studies reported on the causative organisms: Bug Rand Morrey Staph 57% 64% 30% epi Gram neg 13% 12% Strep 8% Anaerobes 4% 6% Mixed 9% 15% MICROBIOLOGY
CLINICAL PRESENTATION • Can be broken down into 3 different time frames: • Early (<2 months) • Intermediate (2 –24 months) • Late (>2 years)
CLINICAL PRESENTATION • Early Infection (<2 months) • Associated with wound healing problems • Persistent drainage • Hematoma • Marginal necrosis • Dehiscence • Often difficult to differentiate between a hematoma and infection
CLINICAL PRESENTATION • Intermediate Infection (2 – 24 months) • Often will have persistent drainage • Key to diagnosis is that they will have pain since the surgery – no pain free interval • Difficult to differentiate RSD from infection
CLINICAL PRESENTATION • Late Infection (>2 years) • Usually spread hematogenously • They has a pain free interval after surgery • Acute: • Fever/Chills, Painful swelling • Insidious: • Decrease motion, Pain at rest vs. ambulation (mechanical)
PLAIN RADIOGRAPHS • Routine evaluation • Usually unremarkable • Nonspecific signs: • Subchondral bone resorption • Periosteal new bone formation • Periprosthetic osteolysis
PLAIN RADIOGRAPHS • The development of a complete radiolucency around a component over a short period of time = infection
LABORATORY TESTS • WBC Count • Usually not elevated • Morrey et al looked at 73 infected TKA’s, only 28% had WBC count > 11,000 • Insall found an average WBC count of 8,300 in infected TKA’s
LABORATORY TESTS • ESR and CRP • Markers of acute inflammation • ESR usually 53 – 63 in TKA infections • ESR elevated in other inflammatory conditions (RA) • ESR has 80% PPV >6 months post-op • CRP normalizes 3-4 weeks post-op
Finland Study on ESR and CRP 40 OA Hips CRP ESR Normal pre-op Elevated pre-op (28) Max POD #2 Max POD #6 (64) Normal POD #21 Elevated at 1 year (30) LABORATORY TESTS
NUCULEAR IMAGING • Bone Scan • 95% Sensitive • 20% Specific • May be positive for 1-2 years post-op • Positive for loose prosthesis • WBC Scan • 84% Accuracy • Expensive
JOINT ASPIRATION • Gold standard for diagnosing infection • Fluid analysis: • WBC >25,000 with 75% PMN’s • Glucose • Normally equal to serum • Decreased in infection • Protein • Normally 1/3 serum • Increased in infection • Gram Stain only positive 25% of the time
JOINT ASPIRATION • Many false negatives and false positives exist • False negatives due to: • Infection localized to bone cement interface • Glycocalyx surrounding bacteria • Antibiotics prior to aspiration • Recommend 2-4 week antibiotic free interval • 72% sensitivity
Gram stain – Notorious for false negative results Only positive 25% of the time Frozen Section – Sensitivity from 7 to 90% Can be a valid test only if appropriate tissue is examined by an experienced pathologist Definition Sensitivity Specificity PPV 5 PMNs/HPF 84% 95.5% 70% 10 PMNs/HPF 84% 99% 89% INTRAOPERATIVE EVALUATION
POLYMERASE CHAIN REACTION • Joint fluid is analyzed • Advantages: • Unaffected by antibiotics • Takes only 4-6 hours • Low cost • PPV 100% • Disadvantage : No bacteriology or sensitivities
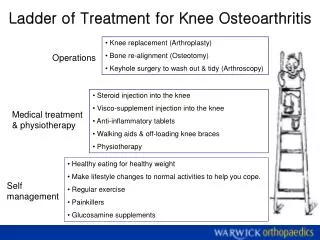
TREATMENT • Six options • Chronic antibiotic suppression • Debridement with prosthesis retention • Resection arthroplasty • Arthrodesis • Amputation • Exchange arthroplasty
CHRONIC ANTIBIOTIC SUPPRESSION • Will not eliminate a deep infection • Criteria: • Poor medical condition • Low virulent organism • Antibiotics needed are low toxicity • Prosthesis well fixed
DEBRIDEMENT WITH PROSTHESIS RETENTION • Criteria: • Short duration of infection (<2-3 weeks) • Susceptible Gram Positive organism • No draining sinus tracts • Well fixed prosthesis • Success in only 20-30% of cases • Best used in early post-op (<4 weeks) – 71% success
RESECTION ARTHROPLASTY • Implies that the implant is removed with no intention of subsequent knee reconstruction • Ideal candidate = polyarticular RA with limited ambulatory demands • Allows patients to sit more readily than with an arthrodesis • Rarely used
ARTHRODESIS • Traditionally the gold standard for treatment of an infected TKA • Indications: • Patient with high functional demands • Single joint disease • Young age • Extensor mechanism disruption • Poor soft tissue envelope • Systemic Immunocompromise • Highly resistant organism
ARTHRODESIS • Contraindications: • Bilateral disease • Severe ipsilateral ankle or hip disease • Severe bone loss • Contralateral extremity amputation • Position : 10-15 deg of flexion
ARTHRODESIS • Types: • Uniplanar Ex-Fix : 33% Union • Biplanar Ex-Fix : 71% Union • IM Nail : 83% Union • Not to be used in active infection
AMPUTATION • Most feared result following infection • Factors leading to amputation: • Multiple revision attempts for infection • Use of hinged prosthesis • Severe bone loss • Intractable pain • Life threatening sepsis • Frequency 5.7% in 1058 infected TKA’s
EXCHANGE ARTHROPLASTY • Direct exchange of implants – most reports demonstrate poor results • Two-stage • Stage 1 – Removal of all implants and cement, debridement of soft tissue • 6 weeks of IV antibiotics • Stage 2 – Reimplant of prosthesis • Debate exists on what to do with the knee for the 6 weeks of antibiotics
EXCHANGE ARTHROPLASTY • Types of “spacers” for the knee • Nothing • Antibiotic impregnated cement spacer • Prosthesis of Antibiotic-Loaded Acrylic Cement (PROSTLAC) • Articulating spacer
EXCHANGE ARTHROPLASTY • Nothing • Has been abandoned because of multiple problems • Contracture of the soft tissue • Extensor mechanism scarring • Instability of knee during antibiotic administration
EXCHANGE ARTHROPLASTY • Antibiotic cement spacer • Spacer serves many roles: • Maintains soft tissue length • Elutes high levels of antibiotics locally • Preserves joint space • 90% success rate • Complications include dislodging of spacer, scarring of quadriceps, and decrease motion
EXCHANGE ARTHROPLASTY • PROSTALAC Spacer • Produced to combat the problems of decreased motion and quadriceps scarring after block spacers • Purpose is to allow mobility and weight bearing between stages, while maintaining adequate soft-tissue tension and joint stability • It is also intended to simplify the reimplantation procedure
EXCHANGE ARTHROPLASTY • PROSTALAC Spacer • First implanted in 1987 – flexible polyethylene mold with cement • Was a high friction system • Fraught with instability
EXCHANGE ARTHROPLASTY • PROSTALAC Spacer • New design decreases friction • Posterior stabilized design
EXCHANGE ARTHROPLASTY • PROSTALAC ROM • Pre – op : 8 – 70 degrees • PROSTALAC implant : 8 – 72 degrees • Final ROM : 5 – 91 degrees
EXCHANGE ARTHROPLASTY • Popularized by Hofmann • Made by cleaning and autoclaving the removed femoral component • This is reinserted during the same operation and articulates with a new tibial polyethylene insert and sometimes a new all-polyethylene patellar component with pegs removed • Cement is mixed with 4.8g tobramycin to 1, 40g batch of cement • Components are placed with cement in a very doughy state
EXCHANGE ARTHROPLASTY • Patients are allowed 50% weight bearing • Allowed to move knee
EXCHANGE ARTHROPLASTY • Components are easily removed at the time of stage II
EXCHANGE ARTHROPLASTY • ROM final 5 – 106 degrees • Compares with other 2 stage protocols • The articulating spacer allows easier reimplantation, improves bone quality, and improves ROM.
CONCLUSIONS • Infection is a feared complication of TKA • Standard treatment is two stage exchange arthroplasty with 6 weeks of IV antibiotics • Antibiotic block spacer has a proven track record • PROSTALAC and Articulating spacers are on the horizon