Download
1 / 34
340 likes | 440 Views
The Urinary System. Functions of the Urinary System. Control plasma electrolyte concentrations Important for maintaining blood osmolarity (_____tonic) Rid the body of waste/metabolites Urea = nitrogen wastes

E N D
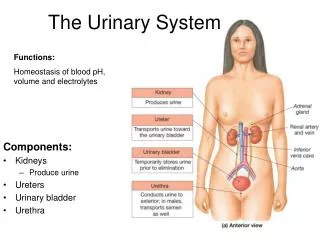
Functions of the Urinary System • Control plasma electrolyte concentrations • Important for maintaining blood osmolarity (_____tonic) • Rid the body of waste/metabolites • Urea = nitrogen wastes • Remember the base product of amino acids = nitrogen base…urea usually reflects nitrogen/amino acid metabolism • Creatinine also reflects amino acid/protein metabolism • Drugs/drug metabolites often excreted in urine as well (urine drug tests) • Help control blood pH • Recall pH homeostasis: kidneys can buffer/control long-term, large changes in blood pH by two mechanisms: • Excrete an acid molecule, recycle bicarbonate/CO2
Functions of the Urinary System • Every cell in your body produces CO2 and other metabolic wastes • Urinary system helps to rid body of waste products • Waste particles are “osmolytes”…they change the tonicity of the blood • Too much waste = too many particles in the blood plasma = hypertonic • Urinary system therefore controls blood osmolarity/tonicity by 2 methods: • Rid body of waste & other particles in the blood • Control the amount of water in the blood
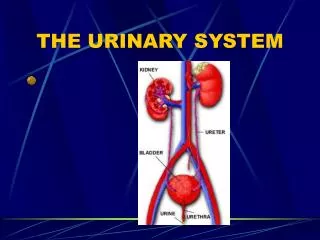
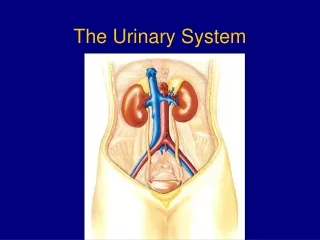
Organs of the Urinary System • Kidneys • Normally paired (developmental malformations can sometimes result in a single kidney…horseshoe kidney) • Very vascular (filters your entire blood volume every 5 minutes) • Vascular supply to-from kidneys • Renal artery & vein • Ureter • Delivers urine to bladder • Bladder • Stores urine until micturation/urination • Urethra • Delivers urine outside the body
Urinary Function • Functional unit = “nephron” • Blood flow is important in terms of nephron function • In order to filter blood, blood has to enter the nephron • Plasma then “pushed” out of a special capillary bed (glomerulus) • Plasma is destined to become “urine” as it is moved down the microscopic tube of the nephron • Nephron = glomerulus & tubule • Urine = blood plasma that has been filtered through the glomerulus (the filter part) of the kidney • As urine passes through the “tubule” (the tube part), various ingredients are re-absorbed by the tube back into the blood
Urinary Function • The shape of the nephron “tube” is important for understanding how this process works • Allows for a mechanism = “countercurrent exchange” • Place a capillary bed very close to one structure, • Allow the blood moving across that structure to take up materials & fluid in a specific order • Changes the tonicity of the blood plasma in the capillary • As blood in the capillary moves over the next structure, it’s tonicity has been altered…will try to restore concentration in the new region by absorbing fluid/water/materials again
Urinary Function • Glomerulus/renal corpuscle is the “filter” of the nephron • Blood enters via “arteriole” (larger and under more pressure than a capillary) • Higher pressure allows for more plasma to be “squished” from the glomerular capillary bed • Plasma crosses into the lumen of the nephron (into the tubule) • Special cells actually help this process • Wrap around the glomerulus capillary bed • “Podocytes” actually help to INCREASE flow into the tubule
The podocyte structure is akin to the astrocytes in the blood – brain barrier. The podocytes & astrocytes wrap themselves around the capillary bed in their respective region. In the nephron, the podocytes allow MORE plasma to filter through than the astrocytes in the brain.
Urinary Function • As the plasma filtrate/urine passes through the tube of the nephron, various regions will re-absorb specific ingredients back into the blood • Proximal tubule = initial region • Re-absorbs nutrients, proteins & electrolytes • Secretes urea/ammonia • Nephron loop (loof of Henle) = middle of the tube • Re-absorbs water • Distal tubule = last region before the “collecting duct” • Re-absorbs water OR • Allows water loss • Also helps to secrete drug metabolites
URINE Idealized tubule
Urinary Function • Surrounding this nephron is a capillary bed • This capillary bed is what allows the “countercurrent exchange” mechanism • Note how the capillary bed makes blood pass over 1 part of the tubule FIRST, then the other part of the tubule SECOND • The regions of the tubule carry out different tasks (transport either water or electrolytes/solutes)
Proximal Distal glomerulus Active transport: electrolytes, glucose, proteins etc. “osmotic drag” of water Water-diluted blood, now iso-osmotic “Concentrated” (plasma has been filtered out at glomerulus) Slightly hypertonic, “extra-concentrated” capillary network
Nephron By making blood hypertonic, there is a water deficit that must be restored in order to maintain homeostasis
PCT DCT Active transport: electrolytes, glucose, proteins etc. “osmotic drag” of water Water-diluted blood, now isotonic “Concentrated” (plasma has been filtered out at glomerulus) Hypertonic plasma
Blood Pressure Control • By adjusting the amount of water that is re-absorbed back into the blood, the kidneys control blood pressure • Re-absorb more water = maintain blood pressure • Allow more water to remain in the tubule (remain in the urine) = reduce blood pressure • Like letting air out of a tire • “anti-diuretic hormone” made in the hypothalamus, stored in the neurohypophysis (posterior pituitary gland) • Acts to increase water re-absorption to maintain blood pressure • Remember the aquaporin water channel? • ADH stimulated the distal tubule to make more aquaporins = more water re-uptake back into the blood
Blood Pressure Control • Aldosterone is another “water retention” hormone • Secreted by the adrenal gland (outer cortex mineralcorticoid) • Stimulates distal tubule to re-absorb sodium • Recall when you absorb an electrolyte, water has to follow • Also stimulates anti-diuretic hormone release (acts in synergy with ADH to increase water retention/re-absorption)
Blood Pressure Control • Angiotensin = another blood pressure “increasing” hormone • Hormone created within the kidneys as well as the lungs • Acts to constrict the blood vessels (vasoconstriction) • In nephron, acts to increase sodium ion re-absorption (similar to aldosterone) • Angiotensin-converting enzymeactivates angiotensin (normally made as a pre-enzyme…not functional until a metabolic enzyme pathway digests it) • ACE-inhibitor medications inhibit this enzyme…increase water loss in the kidneys by lowering the amount of “active” angiotensin in the blood
Blood Pressure Control • Atrial Natiuretic Peptide = hormone made in the atria of the heart • Inhibits electrolyte re-absorption back into the blood • Reduces the osmotic gradient to “draw” water from the tubule back into the blood • Essentially reduces the hypertonic effect • Allowing water to remain in the tubule = water into URINE • Water loss = lower blood pressure
Blood Pressure Control • “Loop diuretics” target the loop of Henle/distal tubule to inhibit water re-absorption • Allows water to remain in the tubule/urine • This is how blood pressure medications work to reduce blood pressure
Blood Pressure Control • The kidneys can only control blood pressure through water/electrolyte re-absorption • If you drastically change the amount of water in your blood, without the correct amount of electrolytes, the kidneys cannot compensate • You only have a “set” amount of sodium, potassium (electrolytes) in your blood • This is dictated by your kidneys…they maintain a homeostatic amount of electrolytes in your blood
Blood Pressure Control • If you lose water, you have to lose electrolytes as well • If you do not lose electrolytes when you lose water, your blood will get hypertonic (too many electrolytes/solutes in the blood plasma) • When you sweat, you lose water AND electrolytes • Hence, after a race, you’re dehydrated (no water) = low blood pressure • BUT, your blood is still isotonic because you’ve sweat some electrolytes (and your kidneys have “lost” some for you as well) • Ingest/inject water without electrolytes = trouble…no electrolytes left to restore isotonicity
Urinary Flow • As the filtered and re-absorbed plasma passes out of the distal tubule, it is now called “urine” • At this point, all the nephrons that make up the kidney will “merge” their “collecting ducts” • Series of larger and larger funnels to collect the urine from all the nephrons in the kidney • Over 4 million nephons per kidney! • Urine then passes through the ureter (tube that transfers urine to the bladder) • Within the bladder, urine is stored until released (micturation/urination)
As urine fills the bladder, the bladder distends (expands) up to 1.5 liters! The “detrusor muscle” sends sensory signals to the brain telling you that you have to go You can “hold it” because of an “external urethral sphincter” that is skeletal muscle (voluntary control)
Note how short the female urethra is (NOT the ureter). This short structure is why females tend to suffer bladder infections more often than males. (remember the estuchian canal in children?) Why females have a more difficult time “holding it” in: the female external urethral sphincter wraps/encloses not only the urethra, but also the vagina…larger area to “close off” makes it harder to hold everything in!
Nephrolithiasis (Kidney Stones) • Kidney stones are hard pellets formed in the nephron as minerals crystallize in the tubule. • Calcium oxalate stones ( 70-80%) • Uric acid ( 7%) • Magnesium ammonium phosphate ( 2%) • Other (xanthine, cystine) ( 2%)
Nephrolithiasis (Kidney Stones) • If permitted to nucleate large enough, stones can lodge in the lumen of nephron and lead to urinary blockade, infection, nephritic damage, and severe pain. • 70-80% of the crystallized minerals from which stones can nucleate are actually passed out in urine without being noticed. • Stones can lodge ANYWHERE along the urinary pathway • Nephron, ureter, bladder & urethra
Polycystic Kidney Disease (PKD) • Genetic disease resulting in gradual kidney degeneration due to cyst formation within the nephron • Etiology is still being studied • Linked to defective transporters along the nephron & absence of primary cilium among others
Renal Dialysis • Should urinary system fail, renal dialysis is an option • Either mechanical or through the use of patients own peritoneal cavity
Renal Dialysis • Chronic ambulatory peritoneal dialysis (CAPD) uses the patients peritoneal membrane as the filtration medium • Introduce dialysis fluid into the peritoneum, withdraw when it has “exchanged” and is full of metabolic waste (4-6 times daily)