Download
1 / 22
400 likes | 2.13k Views
Hypothyroidism. Dr Fidelma Dunne Senior Lecturer Department of Medicine UCHG. Synthesis and Secretion. Follicular cells arranged in clumps. Clumps of cells contain colloid. Colloid an iodine containing protein called thryoglobulin. This is the precursor and storage form of thyroid hormone.

E N D
Hypothyroidism Dr Fidelma Dunne Senior Lecturer Department of Medicine UCHG
Synthesis and Secretion • Follicular cells arranged in clumps. • Clumps of cells contain colloid. • Colloid an iodine containing protein called thryoglobulin. This is the precursor and storage form of thyroid hormone. • Thyroxine (T4), Triiodothyronone (T3)
Thyroid hormone action • T4 and T3 circulate in the blood bound to plasma proteins. • TBG(70%), TBPA(20%) and albumin(10%). • T3 is the active form, 5 times more active than T4. • T4 is converted to T3 outside the thyroid, mostly in liver and kidney. • T3 binds to a nuclear receptor
Regulation of the H-P-T axis • TRH secreted from hypothalmus controls TSH production. • TSH from anterior pituitary stimulates secretion of T4 and T3 from thyroid. • Regulated by a negative feedback loop.
Prevalence of Hypothyroidism • Prevalence is 14/1000 females and 1/1000 males. • Other autoimmune diseases. • Family history of autoimmune diseases
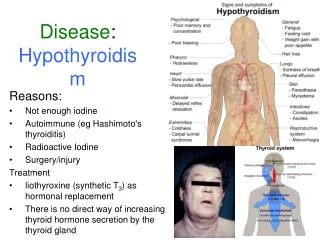
Primary hypothyroidism-Causes • Autoimmune thyroiditis (Hashimoto’s) • Radioactive iodine • Post thyroidectomy • Anti-thyroid drugs (CMZ PTU) • Lithium Amioderone • Iodine deficiency • Subacute thyroiditis • Infiltrative disease • Agenesis
Secondary hypothyroidism-causes • Hypothalamic disease • Pituitary disease
Tiredness Weight gain Cold intolerance Goitre Constipation Bradycardia Angina Cardiac Failure Pericardial effusion Clinical featuresGeneral and CVS
Aches and Pains Carpal Tunnel Deafness Hoarseness Ataxia Depression Psychosis Iron deficiency A Pernicious Anemia Clinical FeaturesNeurological and Haematological
Dry skin Erythema ab igne Vitiligo Infertility Menorrhagia Galactorrhoea Clinical FeaturesSkin and Reproduction
Laboratory Diagnosis • T4/FT4 reduced • T3/FT3 • TSH elevated • Thyroid Antibodies may indicate aetiology. • If TSH is reduced or normal in the presence of a low T4, pituitary function necessary.
Additional abnormal tests. • Fasting cholesterol and triglycerides may be raised • Ck AST and LDH (SMAC 20) may be raised • FBC Anemia • ECG Slow rate. Small complexes.
Treatment • Thyroxine. Usual maintenance dose is 150ug. • Compliance and adequacy of dose checked by TSH measurements. • Try to maintain TSH in normal range.
Subclinical Hypothyroidism • Primary thyroidal failure (Hashimotos) is a gradual process. • Non specific symptoms • Reduced thyroid activity has been compensated by an increase TSH output to maintain a euthyroid state. • Normal T4/FT4 with elevated TSH. • Thyroid antibodies usually positive
Treatment • Repeat tests after an interval. • If TSH is continuing to rise in the presence of strongly positive antibodies, the risk of developing hypothyroidism in the future is high. Thus treatment with thyroxine at this early stage may be justified if symptomatic. • Beware-Thyroxine may not cure all symptoms.
Myxoedema Coma • Requires prompt treatment. Mortality of 50%. • Suspect in cases of hypothermia. • T3 20ug bd IM • Steroids recommended • Glucose to correct hypoglycaemia • Rewarming • Assisted ventilation
Thyroid hormone deficiency in Pregnancy • Goitre is common in pregnant women (70%). • TBG increased, thus total T4 and T3 increased. FT4 and FT3 are normal and TSH remains unchanged. • Hypothyroidism treated with thyroxine during pregnancy. Dose requirements increase. A change in dose usually needed each trimester.
Post-partum thyroiditis. • Incidence is about 9%. • Transitory or permanent. • Early hyperthyroidism (<4/12), later hypothyroidism (>4/12), euthyroid 10/12 later. • Increased microsomal antibodies. • Thyroxine
Elderly • Non specific symptoms • Osteoporosis • Anemia • Heart Failure • Treatment with thyroxine • Start with small doses and titrate slowly. (25ug).
TFTs in severely ill patientsSick euthyroid syndrome • A low serum T4 due to abnormality of binding to serum proteins. • A low serum T3 due to reduced production. • TSH normal • Clinically euthyroid.
Summary • Suspicion • Women • Previous thyroid disease or treatment • Other autoimmune diseases. • Elderly- caution with treatment