Download
1 / 25
410 likes | 1.4k Views
Hypothyroidism. By: Elias S. Hypothyroidism. A common disorder associated with thyroid hormone deficiency resulting from a defect anywhere in the hypothalamic-pituitary-thyroid axis Majority primary thyroid D. Less common TSH , TRH Prevalence U.S. NHANES III on 17353 persons

E N D
Hypothyroidism By: Elias S.
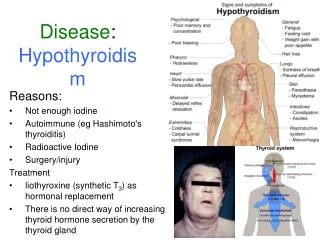
Hypothyroidism • A common disorder associated with thyroid hormone deficiency resulting from a defect anywhere in the hypothalamic-pituitary-thyroid axis • Majority primary thyroid D. • Less common TSH , TRH • Prevalence • U.S. NHANES III on 17353 persons hypothyroidism… 4.6% (subclinical 4.3%, overt 0.3%) • international 2-5% ( to 15% by the age of 75) • Autoimmune Hypothyroidism annual incidence: 4/1000 women, 1/1000 men
Prevalence cont……. • Age: … with age • More prevalent in elderly • Autoimmune hypoth.- Mean age at Dx- 60. • sex: women >(5-8x) Men Framingham study in adults>60yrs 5.9%-women 2.4%- men Race: more common-Japanese NHASESIII, U.S whites(5.1%)>Hispanic A.(4.1%)>African A(1.7%)
causes • Worldwide: • iodine deficiency most common cause • In areas of iodine sufficiency • Autoimmune thyroiditis (Hashimoto’s) • Iatrogenic causes • Hypothyroidism - Primary H. - Central (secondary/tertiary) • Primary hypothyroidism – 2 forms Subclinical Overt( clinical) (TSH, N FT4,N FT3) (TSH, FT4,FT3)
Autoimmune hypothyroidism • Ch. Autoimmune thyroiditis (Hashimoto’s thyroiditis) • Caused by cell-and Ab mediatd destruction of thyroid tissue • Both humoral and cellular factors contribute • Cytotxic T cells • Auto Abs.. TPO 95%, Tg 60%, TSH-R bloking Ab 20%, TBII 10-20% • Two formsHashimoto’s(goitrous)thyroiditis Atrophic thyroiditis
Hashimotos (goitruos)thyroiditis Marked lymph.infiltration Atrophy of thyroid follicles with absence of colloid Mild to moderate fibrosis Present with goiter Minimal or no Sx Atrophic thyroiditis fibrosis Less lymph. infiltration Thyroid follicles completely absent Late stage of Hashimotos thyroiditis Minimal residual thyroid tissue Overt symptoms
Risk factors • Genetic suseptibility • Polymorphism in: HLA DR3,-DR4,-DR5 • CTLA-4(a T-cell regulating gene) • in down’s S., Turners S. • Env. Factors • High iodine intake • infection: congenital rubella s. - autoimmune H. • Cigarette smoking
Iatrogenic causes • Thyroidectomy • 1-4wks after total thyroidectomy • In the 1st yr in the majority of subtotal t. If euthyroid at one year, 0.5-1% chance of hypothyroidism each year • Radioiodine(I-131)therapy • Months to yrs later • Dose dependant • External neck/Total body irradiations • Anti-thyroid drugs (over Rx of Hyperth.)
Other causes • Iodine deficiency • Iodine excess (the wolf-chaikoff effect) • Drugs – Ethanolamine, Lithium, Amiodarone, INF-alpha, IL2 • In Hypothyroid P’ts taking T4: Chlestyramine,Iron salts - T4 absorption Rifampin, Phenytoin,Carbamazepin- clearance Amiodarone, glucocotricoids - conversion of T4T3
Other causes cont… • Infiltrative diseases – rare • Fibrous thyroiditis(reidel’s th.),hemochromatosis,scleroderma, leukemia,amyloidosis • Infections: Tbc., P.carini • Subacut thyroiditis (De-quervain’s,granulomatous) • Silent(painless)thyroiditis –postpartum th. ESR -ve TPOAB Normal ESR, +TPOAb
Secondary/tertiary Hypothyroidism(Central) • <1% • TSH or TRH • Dx – inappropriatly low(low or N. TSH) low T4 and T3 • Causes • Hypopituitarism(tumor,surgery irradiation,sheehan’s s.,hypophysitis) • Mutations in TSH/TSH-R gene • Hypothalamic Damage (tumor,trauma,radiation,inf. D.) • Mutations in TRH-R gene • Drugs – Dopamine, lithium • Dx - MRI
Congenital hypothyroidism • 1:4000 newborns • Thyroid g. agenesis 80-85% • Inborn errors of thyroid H. synthesis 10-15% • TSH-R Ab mediated(Moinfant) 5% • Anti-thyroid (Moinfant) • Majority – appear normal at birth • <10% - prolonged jaundice,feeding problem,hypotonia,enlarged tongue,delayed bone maturation, unblical H., cong.Malf. • Permanent neurologeic D. – if Rx is delayed
Neurologic manifestations • Mental state, poor concentration • Poor memory , emotional lability • Carpal tunnel S. (25-30%) • Cerebellar ataxia (10-30%) • Peripheral neuropathy • Proximal muscle weakness • Hashimoto’s encephalopathy • Myxedema coma
Metabolic Abnormalities • Hyponatremia • Hyperlipidemia (LDL, cholesterol) • Hyperuricemia (Gout) • serum creatinin • carotenemia • drug clearance drug toxicity
High TSH 1° hypothyroidism Non-thyroidal illness(5%) Drugs: Dopamin antagonists, Amiodarone, cholecystographic dyes TSH-producing pit. Adenoma Adrenal insufficiency Thyroid homone resistance S. Low TSH 1° Hyperthyroidism Incomplete recovery from Hyperthyroidism Non-thyroidal illness (10%) High HCG (early pregnancy, molar P., choriocarcinoma) Central hypothyroidism Drugs: Dopamin, Glucocorticoids Somatostatin analogues Phenytoin disorders that affect TSH
Other investigations • CBC, ESR • OFT, Electrolytes • Lipid profile • Uric acid • FNA • Central hypothyroidism • Imaging studies(sellar/supracellar) • Other hormonal profiles (pituitary)
Treatment • Most P’ts …. Require lifelong Rx • The Goals Restoration of euthyroid State Reversion of Sx &Sns Reduction of gotre • Rx thyroid hormone replacement • Synthetic thyroxin(T4) • A pro-hormone, 80% absorbed • Active hormone production controlled by the patient’s own physiologic Mech. • Long half-life(7days) • Once daily when steady state is reached • Should be taken in an empty stomach
Replacement dose • Adults <60 with out evidence of Heart D. • 1.6 mcg/kg/day (50-150) • Older p’ts , p’ts with CHD • 1/2-1/4 of the dose(25-50mcg) • P’t evaluation every 3-6wks • Measure T4(early phase), TSH • Dose adjustment by 12.5-25 ( or ) • Once steady state is reached • Maintenance dose, yearly evaluation with TSH
Additionaladjustment • dose: Pregnancy Estrogen Rx Nephrotic syndrom coadministration of drugs that clearance orabsorbtion • dose: elderly marked w’t loss androgen therapy
?T3 ?T3+T4 • Not recommended • Wide fluctuations of serum T3 conc. • Multiple daily doses • Serum T4 remains low • T3+T4 therapy • For some hypothyroid p’ts who remain symptomatic despite Rx + normal TSH • Meta-analysis of 11 trials No benefit
Central Hypothyroidism • Think of other hormonal deficiencies • T4 Rx to p’ts with untreard 2° adrenal insuficiency acut adrenal crisis! • Glucocorticoid with T4 Rx if adr. Insuff. • Need less T4 than 1°hypothyroidism • Rx monitoring by- FT4 (TSH – no value)