Download

1 / 39
550 likes | 2.23k Views
Hypothyroidism. Katherine Stanley, MD January 14, 2008. Definitions. Overt hypothyroidism: serum TSH above upper limit of normal, free T4 below lower limit Subclinical hypothyroidism- serum TSH above upper limit, free T4 in normal range. Epidemiology 1. Subclinical 5% of adults

E N D
Hypothyroidism Katherine Stanley, MD January 14, 2008
Definitions • Overt hypothyroidism: serum TSH above upper limit of normal, free T4 below lower limit • Subclinical hypothyroidism- serum TSH above upper limit, free T4 in normal range
Epidemiology1 • Subclinical 5% of adults • Overt 0.1-2% of adults • 2% of adolescents (subclinical and overt) • 5-8x more common in women • Congenital HT in 1:4000 newborns
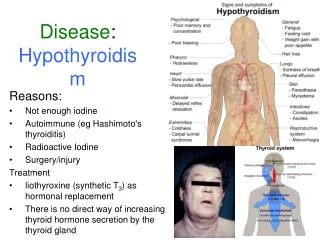
Clinical Manifestations • Constitutional • Fatigue, weight gain, cold intolerance • Skin • Coarse hair and skin, brittle nails, puffy facies, nonpitting edema • HEENT • Enlargement of tongue, periorbital edema, hoarseness
Clinical Manifestations • Cardiovascular • Bradycardia, decreased contractility, increased SVR->incr diastolic BP, increased cholesterol (2x the general population)2, increased homocysteine, pericardial effusions • Respiratory • DOE, rhinitis, decreased exercise capacity, OSA (macroglossia), pleural effusions
Clinical Manifestations • GI • Constipation • Heme • Normocytic anemia, macrocytic anemia (pernicious), hypocoagulable state, incr LDH • Renal • Hyponatremia, increased creatinine
Clinical Manifestations • Reproductive • Menstrual irregularities, decreased fertility, incr prolactin, decr libido, ED, delayed ejaculation • Musculoskeletal • Delayed DTRs, myalgias, arthralgias, incr CK, carpal tunnel • Neurologic • Depression, dementia, Hashimoto’s encephalopathy, myxedema coma
A few words about myxedema coma • Presents w/ altered consciousness, hypothermia, hypoglycemia, hyponatremia, hypoventilation, bradycardia, hypotension • Mortality 30-40% • Treatment • IV T4- load 200-400 mcg, f/b 50-100 mcg/day • Use of T3 controversial • Glucorticoids until adrenal insufficiency ruled out
Clinical Manifestations in Children • Most common manifestation is declining growth velocity, short stature • Generally insidious • May be only symptom • Altered school performance • May actually improve in some children • Delayed pubertal development • Enlarged sell turcica 2/2 hyperplasia of thyrotroph cells • Rarely symptomatic • Reversible with therapy
Other reasons to check the TSH • Goiter • Surgery around the thyroid • Irradiation • Drugs that affect thyroid • Lithium, amiodarone • Autoimmune diseases • DM 1, pernicious anemia, vitiligo, primary adrenal insufficiency, PBC • Chromosomal disorders, eg Down’s, Turner’s, Klinefelter’s
Causes of Hypothyroidism • Chronic autoimmune thyroiditis (Hashimoto’s) • Most common cause in both children and adults • Thyroidectomy • 2-4 weeks with total, variable with subtotal • Neck irradiation • Radioiodine therapy • Iodine- deficiency or excess • Drugs • Lithium, amiodarone, kelp, IFN-a, IL-2, contrast • Infiltrative disease
Hypothyroidism in Childhood Cancer Survivors • One study found that 36% of childhood cancer survivors had developed primary HT, 32% central/mixed3 • Major risk is from radiation to head and neck • Current guidelines recommend yearly TSH and T4 in such patients4 • May be some risk from chemo alone • 30% of the patients in above study had not received any radiation
Diagnosis • Check the TSH • 98% sensitive, 92% specific • Why is TSH the best test? • T4 has wide range of normal • Everyone has endogenous optimum set point • TSH will increase when fall below set point • If TSH increased, check free T4
Tricky Thyroid- when TSH doesn’t work • Secondary/Tertiary Hypothyroidism • TSH can be low, inappropriately nl, or slightly high (biologically inactive) • Check FT4 if suspect • Suspect if: known hypothalamic or pituitary dz, prior cranial irradiation, mass lesion in pituitary, s/sx of other hormonal deficiencies • Drugs that affect Thyroid Testing • See next slide • Don’t forget about sick euthyroid
Drugs and Thyroid Testing • Decreased TSH secretion • Glucocorticoids, dopamine • Decreased TBG • Glucocorticoids, androgens, niacin • Increased TBG • Estrogens, tamoxifen, methadone, heroin, clofibrate • Increased T4 clearance • Phenytoin, carbamazepine, rifampin, phenobarbital • Decreased T4 binding to TBG • Furosemide, heparin, salicylates, NSAIDs
To screen or not to screen? • American Thyroid Association recommends universal screening q5yrs beginning at 355 • High prevalence • Known clinical consequences • Accurate, available, safe, inexpensive assay • Effective treatment • Cost effectiveness analysis published in JAMA6 found $9223 per quality adjusted life year (QALY) in women, $22595 per QALY in men, mostly based on relieving sxs associated with thyroid failure
To screen or not to screen? • U.S. Preventive Task Force Guidelines declares evidence insufficient to recommend routine screening7 • Poor evidence that treatment improves clinically important outcomes • Low PPV in primary care population
Treatment • Average required dose is 1.6 mcg/kg • Required dose more closely w/lean body mass than fat mass8 • May want to consider dosing closer to ideal body weight in obese pts
Treatment in children • Children clear T4 more rapidly than adults • Age 1-3: 4-6 mcg/kg • Age 3-10: 3-5 mcg/kg • Age 10-16 2-4 mcg/kg • Avoid overtreatment • Maintain TSH in lower nl range, T4 in upper normal • Can cause craniosynostosis in infants, deleterious effects on behavior, school performance, growth • May spontaneously remit, but should continue treatment until complete growth and puberty
Start low, go slow? • Some physicians adhere to this principal in all pts • RCT comparing full dose vs. low starting dose of 25 mcg9 • Excluded pts with known cardiac disease • Everyone remaining screened with dobutamine stress echos • Full dose group reached euthyroidism more quickly • No cardiac events in either group • No difference in rate of QOL improvement or cholesterol improvement
So… • Pts older than 65, known cardiac disease should start at 25 mcg • Young, healthy patients should start at full dose (1.6 mcg/kg) • Check TSH 3-6 wks after starting and after any changes
What brand should I use? • Bioequivalence studies of Synthroid, Levoxyl, and 2 generic preps showed no significant differences for area under curve, time to peak, peak conc of T3, T4, and FTI10 • However, FDA recommends remaining on same preparation, checking TSH after 6 wks if pt must change11
What if my patient won’t take their Synthroid? • T4 has very long half life • Can give total weekly dose qwk12 • Caveat- above recommendation based on small, relatively short study
What if my pt wants more Synthroid? • Pts often say they feel better on higher doses which put their TSH in lower range of normal, even a bit hyperthyroid • Double blind crossover study comparing low, middle, and high doses113 • No difference in quality of life, cognitive measurements when compared both based on dose and TSH level
Special Cases- Cardiac Disease14 • Treatment should improve cholesterol, DBP, contractility • Improves angina in some (38%), 46% have no change, 16% have increased sxs • No evidence of decr CV M&M with tx of hypothyroidism • Some evidence of increased CV M&M when initiating treatment • Generally, start very slowly (25 mcg), consider extensive cardiac assessment, eg stress or angio, and possible medical tx and/or stenting or CABG
Special Cases-Elderly • Another population to start slowly with, perhaps consider not treating • Cohort study addressing disability and survival in old age in relation to thyroid status15 • No difference in mortality rate, decline in cognitive fxn, decline in ability to carry out ADLs and IADLs, depression with increased TSH • May even have decr mortality w/incr TSH • ?Survival benefit
Special Cases- Subclinical16 • TSH 4.5-10, no treatment • Rate of progression 2.6% Ab-, 4.3% Ab+ • Monitor TSH q6-12 mos • TSH >10, consider tx given 5% rate of progression to overt but inconclusive evidence of benefit • Pregnancy, treat given evidence of worsened fetal outcomes • Treated overt, adjust dosage
What if I have SHT and …? • Depression17,19 • No difference in cognitive and emotional fxn between those with SHT (TSH 3.5-10) and without • No difference in above in those with SHT after tx w/T4 vs. placebo • Obesity18,19 • No diff in BMI or body weight after tx of SHT • High cholesterol20,2 • While pts w/SHT may have worse lipid profiles, no beneficial effect of tx has been conclusively shown • Fatigue19 • No difference in impr btw treatment and placebo
Subclinical hypothyroidism in children21 • Baseline TSH less predictive of rate of progression than in adults • Higher baseline thyroglobulin Ab and thyroid volume may be predictive • Increasing TPO Ab over time may be indicative of declining thyroid fxn • No growth retardation in children w/SHT followed over 5 years • Treatment is controversial22,23
Special Cases-Pregnancy • Increased TBG, T4 clearance, and transfer of T4 to fetus • Increased requirement begins @ 8 wks, plateaus @ wk 16 • Consider increasing dose when pregnancy confirmed, then check TSH q4wks until TSH nl
Special Cases-Congenital hypothyroidism • Most common treatable cause of mental retardation • Etiologies • Most common is thyroid dysgenesis • Defects in thyroid hormone synthesis, secretion, and transport • Central- congenital syndromes, birth injury, insufficient tx of maternal hyperthyroidism • Transient-iodine deficiency or exposure, antithyroid drugs, maternal transfer of blocking antibodies
Congenital HT24 • Clinical Manifestations • Lethargy, slow movement, hoarse cry, feeding difficulties, constipation, macroglossia, umbilical hernia, large fontanels, hypotonia, dry skin, hypothermia, prolonged jaundice • But most infants have few if any s/sx • Hence part of newborn screen • Some screens check T4, some check TSH • Advantages and disadvantages of both • Treatment • Oral T4 (crushed pills) • 10-15 mcg/day • Avoid soy formula
Congenital HT • Prognosis • Normal growth, development, and intelligence if treated early (<2 wks) • Improved outcomes with higher initial T4 dose and shortened time to target T4 and TSH25
Special Cases-Drugs affecting Treatment • Drugs that affect TBG or binding of T4 to TBG • I already told you • Drugs that decrease absorption of T4 • Cholestyramine, CaCO3, FeSO4, sucralfate, PPIs, and others
Special Cases- Surgery • Higher incidence of ileus, hypotension, hyponatremia, CNS dysfunction • Consider postponing elective surgeries • Not urgent surgeries, just be aware of slightly increased complications
References 1 Hollowell, JG et al. Serum TSH, T4, and thyroid antibodies in the US population (1988-1994): National Health and Nutrition Examination Survey (NHANES III). JCEM 2002: 489. 2 Diekman, T et al. Prevalence and correction of hypothyroidism in a large cohort of patients referred for dyslipidemia. Arch Intern Med 1995; 155: 1490. 3 Rose, SB et al. Diagnosis of hidden central hypothyroidism in survivors of childhood cancer. JCEM 1999: 4472. 4 Children’s Oncology Group. Long-term follow-up guidelines for survivors of childhood, adolescent, and young adult cancers. National Guidelines Clearinghouse 2006: www.guideline.gov. 5 Ladenson, P et al. American Thyroid Association Guidelines for Detection of Thyroid Dysfunction. Arch Intern Med 2000; 160: 1573. 6 Danesee, MD et al. Screening for mild thyroid failure at the periodic health examination: a decision and cost-effectiveness analysis. JAMA 1996; 276: 285. 7 US Preventive Services Task Force. Screening for thyroid disease: recommendation statement. National Guidelines Clearinghouse 2004: www.guideline.gov. 8 Santini, F et al. Lean body mass is a major determinant of levothyroxine dosage in the treatment of thyroid diseases. JCEM 2005; 90-: 124. 9 Roos, A et al. The starting dose of levothyroxine in primary hypothyroidism treatment: a prospective, randomized, double-blind trial. Arch Intern Med 2005; 165: 1714. 10 Dong, BJ et al. Bioequivalence of generic and brand-name levothyroxine products in the treatment of hypothyroidism. JAMA 1997: 277: 1205. 11 Joint statement on the U.S Food and Drug Administration’s decision regarding bioequivalence of levothyroxine sodium. Thyroid 2004; 14:486. 12 Grebe, SKG et al. Treatment of hypothyroidism with once weekly thyroxine. JCEM 1997; 82: 870. 13 Walsh, JP et al. Small changes in thyroxine dosage do not produce measurable changes in hypothyroid symptoms, well-being, or quality of life: results of a double-blind, randomized clinical trial
References • 14 Feldt-Rasmussen, U. Treatment of hypothyroidism in elderly patients and in patients with cardiac disease. Thyroid 2007; 16: 619. • 15 Gussekloo J. Thyroid Status, disability and cognitive function, and survival in old age. JAMA 2004; 292: 2591. • 16 Subclinical thyroid disease: scientific review and guidelines for diagnosis and management. National Guidelines Clearinghouse 2004. www.guideline.gov. • 17 Jorde, et al. Neuropsychological function and symptoms in subjects with subclinical hypothyroidism and the effect of thyroxine treatment. JCEM 2006; 91: 145. • 18 Portmann L. Obesity and hypothyroidism: myth or reality? Revue Medicale Suisse 2007; 105: 859. • 19 Kong, WK, et al. A 6-month randomized trial of thyroxine treatment in women with mild subclinical hypothyroidism. Am J Med. 2002; 112: 348. • 20 Pearce, EN. Hypothyroidism and dyslipidemia: modern concepts and approaches. Current Cardiology Reports 2004; 6: 451. • 21 Radetti G. et al. The natural history of euthyroid Hashimoto’s thyroiditis in children. J Pediatr. 2006; 149: 827. • 22 Fatourechi, Vahab. Subclinical hypothryoidism: how should it be managed? Treatments in Endocrinology 2002; 1: 211. • 23 Moore, DC. Natural course of ‘subclinical’ hypothyroidism in childhood and adolescence. Arch Pediatr Adolesc Med 1996; 150: 293. • 24 Rose, SR et al. Update of newborn screening and therapy for congenital hypothyroidism. Pediatrics 2006; 117:2290.
References • 25 Selva, KA et al. Neurodevelopmental outcomes in congenital hypothyroidism: comparison of initial T4 dose and time to reach target T4 and TSH. J Pediatr 2005; 147: 775. • 26 Surks, M. Clinical manifestations of hypothyroidism. www.utdol.com. • 27 Ross, DS. Diagnosis of and screening for hypothyroidism. www.utdol.com. • 28 Ross, DS. Treatment of hypothyroidism. www.utdol.com. • 29 Green, GB. Hypothyroidism. Washington Manual of Medical Therapeutics. Lippincott Williams & Wilkins, Philadelphia, 2004: 489-492. • 30 Ross, DS. Myxedema coma. www.utdol.com • 31 LaFranchi, S. Acquired hypothyroidism in childhood and adolescence. www.utdol.com • 32 LaFranchi, S. Clnical features and detection of congenital hypothyroidism. www.utdol.com • 33 LaFranchi, S. Treatment and prognosis of congenital hypothyroidism. www.utdol.com