Download
1 / 49
490 likes | 587 Views
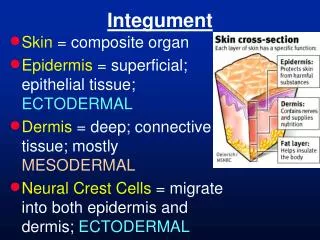
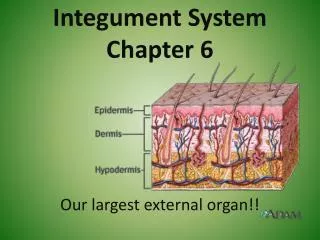
The Integument System. The skin & associated disorders NUR 331 On-line study self-study Dr. Sara Mitchell. Purposes of the skin. Protection Impermeability Heat regulation Sensation. Purposes of the skin. Protection

E N D
The Integument System The skin & associated disorders NUR 331 On-line study self-study Dr. Sara Mitchell
Purposes of the skin • Protection • Impermeability • Heat regulation • Sensation
Purposes of the skin • Protection • Protects against trauma, including mechanical, thermal, chemical, & radiant • Protects by the oily slightly acid secretions of the sebaceous glands which limit the growth of bacteria
Purposes of the skin • Impermeability • Seals the skin from the environment • Protects against loss of essential body constituents to the environment.
Purposes of the skin • Heat regulation • Skin adjusts heat loss to heat production to maintain the thermal balance of the body.
Purposes of the skin • Sensation • Perceptions (touch, pain, heat, cold) are transmitted through the nerves that permeate the skin. • Betrays emotions/feelings
What makes skin in children different? • Eccrine glands do not reach mature function until 2-3 years of age. • Skin is more alkaline in the first weeks of life. • Subcutaneous fat is poorly developed. • The newborn’s skin is thin an friable. • IgA is decreased until 2-5 years of age.
What makes skin in children different? • Lack of maturity of eccrine glands makes infants & young children less able to regulate body temperature • Decreased SQ fat predisposes to hypothermia • Thin skin makes it more susceptible to external irritants and to infection
Test your knowledge 1. Purposes of the skin include _______, ______, _________, and ____________. 2. The skin adjusts heat loss to heat production to maintain the _______ _____ of the body. 3. Skin in children is different because of which of the following? A. skin is more acidic in the first few weeks of life B. IgA is increased until around 2-5 years of age C. Decreased SQ fat predisposes to hypothermia • 1. protection ,impermeability, heat regulation, sensation 2. thermal balance 3. C
Test Your Knowledge Read pages 758-768 and answer the following questions: 4. Which of the following factors hinder wound healing? A. Dry wound environment B. Nutritional deficiencies C. Impaired circulation D. all of the above 5. Which of the following factors aids in wound healing? A. Leaving wound open to dry out B. Cleaning with hydrogen peroxide and betadine C. Cooling the affected area 4. D 5. C
Test your knowledge 6. The major nursing function related to bacterial skin infections are to prevent the spread of infection and to prevent complications. • A. True • B. False 7. Most communicable diseases of childhood are associated with ______ caused by ________. 6. A 7. rashes/viruses
Infections of the skinCaused by bacteria • The major nursing functions related to bacterial skin infections are to prevent the spread of infection and to prevent complications.
Bacterial Infections - Name a few(see page 767 in textbook) • Impetigo • Cause • Course • Management • Caution • Cellulitis • See page 767 in your textbook and figure 18-7 on page 767
What causes impetigo and how does it progress? • Caused by group A beta hemolytic and/or staph aureous • Course is as follows: • Begins as a single reddish maculae, then becomes vesicular • Ruptures easily, leaving superficial moist erosion • Tends to spread peripherally • Exudate dries to form a heavy honey-colored crust
Impetigo: How is it managed? • Gentle washing with soap and water • Apply topical antibiotic ointment • May occasionally need oral antibiotics • Antibiotics in the penicillin or cephalosporin family are generally prescribed. Erythromycin is used for those allergic to penicillin. • Impetigo is VERY contagious • Children diagnosed with impetigo should be instructed to stay home from daycare/school for 24 hours after beginning medications
Test your knowledge • Joey is a 7-year-old boy who comes to the school nurse’s office with the complaint of itchy rash on his face. As the school nurse, you assess the rash to be reddened papules and pustules with a yellow crust occurring around his mouth and nose. • 8. What is your firstpriority • A. Assess his temperature and lung sounds • B. Have the child wash his hands and call his parents to have Joey see the doctor • C. Apply calamine lotion to the affected areas • D. All of the above. • 9. Which of the following statement demonstrates effective learning by Joey’s parents regarding his treatment? • A. “I should keep Joey’s towels separate from my other children.” • B. “Joey should bath in Aveeno baths at night to help with the itching.” • C. “I should wash Joey’s linen in hot water and soak his combs in boiling water.” • D. “Joey should take Acyclovir until all of the lesions are gone.” 8. B 9.A
Infections of the skinCaused by viral agents • Most communicable diseases of childhood are associated with rashes caused by viruses
Viral skin infections :Name a few • Warts • Caused by human papillomavirus • Occurs anywhere but usually appear on exposed areas such as fingers, hands, face, and soles of feet. • Hard to get rid of. Tend to disappear spontaneously • Treatment includes cryotherapy, surgical removal, or salicyclic acid
More viral skin infections • Herpes simplex virus • Type I – causes clod sores & fever blisters • Type II – causes genital lesions and is sexually transmitted • Management directed toward keeping lesions moist with burrows solution. Topical or antivirals may be used. Lesions are made worse by steroids. May be fatal in children with decreased immunity.
Test your knowledge • 10. Treatment for warts includes which of the following? • A. cryotherapy • B. surgical removal • C. salicylic acid • D. all of the above • 11. Warts are caused by the human herpes virus. • A. True • B. False • 12. Children with ringworm should be instructed to avoid contact with other children for how long after treatment has begun? • A. 1 day • B. 2 days • C. 3 days • D. It doesn't matter 10. D; 11. B; 12. B
Another skin eruption caused by a virusVaricella-also known as Chicken Pox • What causes it? • varicella zoster viruses • When does it generally occur? • Most often occurs in late winter and early spring • How is it spread? • It is spread by direct contact and droplet (airborne) transmission
More on Chicken Pox • Is Chicken Pox contagious? • It is very contagious. It can be spread starting 1-2 days before eruption of lesions and until the time when all lesions have crusted. • When can children return to school or day care? • Not until ALL lesions have crusted which is usually about 1 week. • It is not necessary to wait until all the scabs fall off to let the child return to a normal schedule
Chicken Pox – Sign & Symptoms • Red, itchy rash on skin. • Rash begins as small, red bumps that look like pimples or insect bites. • Red bumps develop into thin-walled blisters filled with clear fluid, which becomes cloudy • Blisters break, leaving open sores, which finally crust over to become dry, brown scabs. • Fever 100-1020F (may occasionally be higher)
Chicken Pox – about the rash • Lesions erupt in successive crops, usually beginning on the trunk and then spreading to the face and scalp. • The characteristic rash involves crops of teardrop vesicles on an erythematous base. • The classic lesion has been described as an "oval teardrop on an erythematous base" or a "dew drop on a rose petal.“ • A characteristic feature of the rash is that the lesions can be in all stages of development simultaneously.
Chicken Pox – what is the Incubation period? • The incubation period for chicken pox is 10 to 21 days after exposure. • Most cases appear within 14 to 17 days. For example, if one child in a family breaks out with chickenpox picked up at school, siblings probably will show symptoms about 2 weeks later.
ChickenPox – What is the treatment • Relieve the itch! • Cool or tepid oatmeal baths with every 3 to 4 hours as needed (baths do not spread chickenpox) • Calamine lotion (avoid the face, especially the eyes) • Antihistamines, such as benadryl, may also be used for itching • Soft/bland foods as indicated as there may be painful pox lesions in the mouth • Acetaminophen or ibuprofen or fever and general aches • Antiviral medications such as acyclovir may occasionally be prescribed at the physicians discretion
Chicken Pox – What are the complications? • Viral pneumonia • Encephalitis • Secondary skin infection
Chicken Pox – How is it related to shingles? • Anyone who has had chickenpox as a child is at risk shingles later in life. • After infection with chickenpox, some of the varicella zoster virus may remain inactive in the nerve cells near the spinal cord. • Many years later, the virus can reactivate and resurface as shingles. • When it reactivates, it affects the nerves to the skin. • Symptoms, such as a tingling feeling, itching, or pain followed by a rash with red bumps and blisters appear only on the area of the skin that the nerve goes to.
What about the chicken pox vaccinehttp://www.vaccineinformation.org/varicel/qandavax.asp • In use since 1995 • 70-85% effective at preventing mild infection and more than 95% effective in preventing moderate to severe disease. • Given to all children older than 12 months of age, as well as adults who have not had the disease.
Chicken Pox – test your knowledge 13. Tommy has been diagnosed as having chicken pox. His mom ask you how the disease is spread. Your best response is: A. by direct contact with the lesions B. by an infected person breathing on you C. by kissing an infected person D. all of the above 14. Tommy’s best friend has chicken pox. His mom is worried about Tommy getting the disease as well and ask you what the early signs are. Your best response is: • A. Symptoms develop 3-5 days after exposure • B. Lesions usually begin on the trunk • C. The rash begins as small, red bumps that look like pimples • D. B & C • E. A only 13. D; 14. D
Chicken Pox – test your knowledge 15. It has been 10 days since his exposure to chicken pox and Tommy has not developed signs of the disease. His mom ask if he is out of the woods. Your best response is what? • A. It is unlikely Tommy will develop chicken pox from this exposure • B. The incubation period for chicken pox is 5-7 days • C. Most cases of chicken pox appear within 14 to 17 days of exposure. • D. It is impossible to tell if Tommy will develop chicken pox. 16. Tommy does not develop chicken pox but his brother does. Tommy’s mom ask what she should do to treat the disease. Your best response is what? • A. Avoid baths because of risk of causing the pox to spread. • B. Apply calamine lotion for the itch • C. Give acetaminophen for fever and aches • D. A only • E. B & C 15. C; 16. E
Chicken Pox – test your knowledge 17.Tommy’s mom needs to return to work. She ask when her son while likely to able to return to school. Your best response is what? • A. When all of the scabs have fallen off • B. When all lesions have crusted and are no longer fluid filled vesicles • C. When she hasn’t seen any new lesion for 48 hours • D. All of the above • 17. B
Skins infections caused by fungi • Tinea captitis – fungal infection of the scalp • Tinea corporis – fungal infection of the body • Tinea curis – fungal infection of the scrotal and genital area • Tinea pedis -athlete's foot
Skins infections caused by fungi • Management • Skin infections: treated with topical antifungal creams for 6-8 weeks • Scalp infections: because the fungi are deep in the hair shaft tinea capitis must be treated with systemic antifungal medications such as grieseofulvin for 6-weeks • Ringworm is contagious. Children with ringworm should be instructed to avoid contact with other for 48 hours after treatment is started.
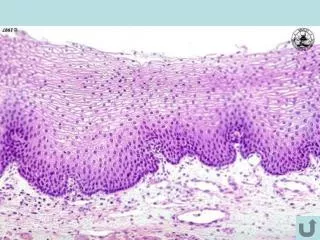
Different forms of tinea – What does it look like? Tinea Capitis Tinea Corporis- face & trunk Tinea cruris – groin, buttocks, & scrotum Tinea Pedis
Scabies • Definition –an endemic infestation caused by the scabies mite sacroptes scabiei. The mite can barely be seen by the naked eye • Clinical manifestations – the mite burrows under the skin causing an allergic reaction. Recognized by their tracks …small lines in the skin that look like scratches about ¼ inch long. Usually appear at wrists, buttocks, underarms, groin, and especially in the webs between fingers and toes. • Therapeutic management – scabicide such as Elimite (5% permethrin) • Nursing considerations – education about transmission and management
Pediculosis capitis:a fancy name for head lice or “cooties” • Definition – an infestation of the scalp by Pediculus humanus capitus • Clinical manifestations –causes intense itching. Very common especially in school children • Therapeutic management – comb nits out. Treat with 1% permethrin shampoo. • Nursing considerations – head lice are very contagious. All family members should be treated. Anything that has come in contact with the scalp, brush, hats, bed linens, ect.. needs to be cleaned
Poison Ivy,Oak, Sumac:itchy, itchy, itchypage 767 in textbook • Definition • A contact dermatitis that occurs when skin comes in contact with the dry or succulent portion of any of the three of these plants. The offending substance is an oil called urushiol • Clinical manifestations • Contact produces localized, streaked, or spotty, oozing and painful impetigious lesions. The substance begins to take effect as soon as it touches the skin. It soaks in and causes an immune response. A full-blown reaction is evident after about 2 days.
The oil contained in the plant leaves irritates the skin. The redness and blistering from the rash is often arranged in streaks or lines, because the leaf brushes across the body in a line as an individual walks past. Poison Ivy Rash –What does it look like?
Poison Ivy,Oak, Sumac:itchy, itchy, itchy (continued) • Therapeutic management • The primary goal of treatment is to lessen the itch and prevent secondary infection. Calamine lotion, baths in aveeno or baking soda are helpful in relieving the itch. Oral benadryl can be used as well as topical hydrocortisone. If the out break is extensive or if it is near the eyes systemic steroids (i.e. prednisone) is often used. • Nursing considerations • Wash area immediately with cold running water to neutralize the urushiol. Remove and wash all clothing that may have come in contact with the plant.
Poison Ivy,Oak, Sumac:itchy, itchy, itchy (continued) • Common myth • Poison ivy, oak, or sumac can not be spread from person to person. There must be contact with the urushiol oil before a contact dermatitis response can occur. Contact can be directly from a plant, from clothing, or perhaps from the fur of a family pet who has been romping in the woods.
Test your knowledge A mother calls the clinic nurse to ask advice regarding her child and possible contact with poison ivy. 18. If the contact was in the last 15 minutes, which of the following actions should be recommended? • A. Wash the child with dishwasher detergent • B. Flush the skin with cold running water • C. Have the child bathe in warm water • D. Have the child shower in hot water. 19. Clothing the child was wearing should be • A. Burned • B. Placed in a plastic bag and put out with the trash • C. Placed in the laundry hamper along with other clothes • D. Washed separately in hot water and detergent • Answers 18. B; 19. D
Prevention Sunscreen and sunblocks. SPF 15 or greater. Avoid mid day sun exposure Treatment Involves stopping the burning process, decreasing the inflammation process, and rehydrating the skin. Cool tap water soaks or immersion in a tepid water bath for 20 minutes or until the skin is cool. Apply moisturizing lotion. Use Tylenol for discomfort. Sunburn:Ochy,Ochy, Ochy
Atopic Dematitis:Ou wee baby • What is it? • Also referred to as eczema. It is a chronic inflammation of the dermis and epidermis which causes itching, edema, papules, erythema, excoriation, serous discharge and crusting. • Who gets it? • * see page 580 in your textbook for the different age groups. There is often a family history of eczema of some other chronic allergy related condition.
Atopic Dematitis:Ou wee baby (continued) • Management • Basic skin care • Frequent baths but also apply moisturizing lotion within three minutes after bath (while the skin is still damp.
Atopic Dematitis:Ou wee baby (continued) • Medications to relieve itch or secondary infection • Topical steroids • Oral antihistamines • Antibiotics for secondary infection • Education, Education, Education! • Parents must understand this is a chronic condition that reoccurs. There is no one time fix. If they do not understand this they will only be frustrated with the medical system for not “curing” their child
Diaper Rash:What are the causes • Caused by a prolonged and repetitive contact with an irritant, i.e. urine, feces, soap, detergents. • Wetness, increased skin Ph, and fecal irritants all work together to cause the rash.
Use zinc oxide paste to help create a moisture barrier so that the irritated skin can heal Clean the area very gently Use a cleanser only after the infant has had a bowel movement Use nonirritating wipes Use super-absorbent diapers. Research has shown that some diapers with super absorbency and petroleum layers helps reduce the incidence of diaper rash Diaper Rash:What is the treatment