Download

1 / 85
850 likes | 858 Views
IMAGING TECHNIQUES IN URINARY SYSTEM. HISTORY. Dates back to 1896 when first X-ray demonstration of renal calculus was done. Subsequently, cystography, retrograde pyelography and retrograde urethrography were developed. In 1929, i.v contrast agent that can be used for IVP- uroselectan.

E N D
HISTORY • Dates back to 1896 when first X-ray demonstration of renal calculus was done. • Subsequently, cystography, retrograde pyelography and retrograde urethrography were developed. • In 1929, i.v contrast agent that can be used for IVP- uroselectan.
Principal use- detection of urinary tract calculi • Extremely unreliable in diagnosis of ureteric calculi.
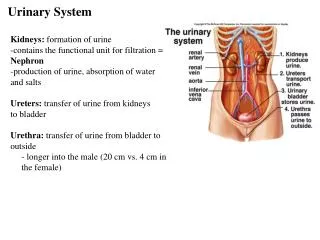
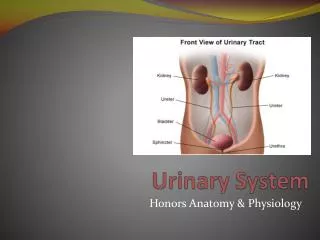
An intravenous urogram (also known as IVU, pyelography, intravenous pyelogram or IVP) is the radiographic examination of the urinary tract including the renal parenchyma, calyces, pelvis, ureters and bladder after the intravenous injection of the contrast media.
Use decreased significantly in recent years. • CT, US, MR is replacing. • Remains primary modality for visualization of pelvicalyceal system and ureter.
Indications • Investigation of Hematuria. • Abnormalities of the ureter. • Obstructive uropathy. • Renal and ureteric calculi (particularly prior to endourological procedures). • Suspected renal injury. • Ureteric fistulas and strictures. • Complex infections like tuberculosis • Suspected urinary tract pathology. • Differentiation of function of both kidneys
Contra Indications • General contra indications to iodinated contrast agents. • Hepatorenal syndrome, • Thyrotoxicosis • Pregnancy, (Allow 28 days from childbirth) • Blood urea raised above 12 mmol ./L. urography unlikely to be successful • Serum creatinine above1.2mg% • History of severe anaphylaxis.
Value of nephrographic analysis • Failure to visualize nephrogram Insufficient dose of contrast Acute or chronic renal failure End stage renal disease Absent kidney Renal artery thrombus / avulsion
Patient preparation • Every radiology department has their own specific requirements. Basic abdominal preparation, to clear fecal residue. • Tab Dulcolax + gasex 2days prior • Nil by mouth for 4-6 hours before the examination. Dehydration is not necessary and does not improve image quality. • Basic psychological preparation with reassurance and explanation of technique & written informed & valid consent • Bladder emptied immediately before examination.
COMPRESSION BAND TECH • Aim :To produce better pelvicalyceal distension • Abdominal compression is applied as soon as the 5 min film has been taken. The balloon is positioned on ASIS where ureters cross pelvic brim. • C/I : After recent surgery Renal trauma Aortic aneurysm Children(Routinely omitted) Acute painful abdomen including renal colic Large abdominal mass • If 5 min film shows dilated calyces or if calyces and pelvis are not adequately opacified, obstruction exists and compression band should not be applied
End of Injection, A.P. of the renal areas to show the nephrogram, i.e. the renal parenchyma opacified homogenously by the contrast medium in the renal tubules.
5 Minute film, A.P. of the renal areas to determine if excretion is symmetricalor if uptake is poor and a further dose of contrast agent is required..
High dose radiography-Used in mild renal impairment • Indications: Renal failure Ureteric obstruction Emergency urography Supra renal tumors Inadequate bowel preparation Percutaneous nephrostomy
Three abnormal time-density patterns are recognized • Immediate, faint & persistent nephrogram • Increasingly dense nephrogram • Immediate, dense & persistent nephrogram
Immediate, faint, persistent nephrogram • Peak density is seen on the first phase at the completion of injection of contrast. • Density is disproportionate with amount of contrast material injected. • Though faint nephrogram persists for several hours.
Seen in : • Chronic glomerular disease • Sudden loss of glomerular function- atheroembolic renal disease These diseases are often associated with a high urea load & impaired sodium reabsorption in PCT- also contribute to faintness of nephrogram.
Immediate faint persistent nephrogram Chronic glomerulonephritis
Increasingly dense nephrogram • Faint to begin with • Increasingly dense over a period of hours to days
Seen in: • Acute extra-renal obstruction • Diminished perfusion pressure of kidney systemic hypotension severe RAS 3. Intratubular obstruction uric acid crystals myeloma casts acute papillary necrosis • Acute renal vein thrombosis • Acute glomerular disease • Acute tubular necrosis
10 min 4 hrs Increasingly dense nephrogram Distal ureteric calculus
Diminished perfusion pressure of kidney- • Systemic arterial hypotension • Severe RAS Pathogenesis- diminished perfusion pressure of kidney Reduction in rate of contrast increased reabsorption clearance from plasma of salt & water by tubules slow accumulation of contrast *In systemic hypotension both kidneys become increasingly dense. *While in severe RAS, it is unilateral.
1 min 15 min Increasingly dense nephrogram Systemic hypotension
Immediate, dense, persistent nephrogram • As dense as normally expected to be at 1 minute • The level of density persists rather than fading away • Often slightly increases over a period of hours to days
Pathogenesis- has not been clarified unimpaired glomerular filtration (immediate dense nephrogram) diffusion of filtrate into interstitium due to damaged tubules return of filtered material to the circulation (persistent nephrogram)
Seen in- • Acute tubular necrosis * if this pattern sets in after an initially normal urogram, suggests contrast induced nephrotoxicity • Acute bacterial nephritis * almost always unilateral
10 min 12 hrs Immediate dense persistent nephrogram Acute tubular necrosis
Inhomogeneous nephrogram- • Striated nephrogram • Patchy nephrogram • Cortical rim nephrogram
Striated nephrogram(Sunburst nephrogram) Def-inhomogeneous tubular nephrogram, characterized by fine linear bands of alternating lucency & density uniformly oriented in direction similar to that of tubules & collecting ducts Pathogenesis- stasis of urine in collecting tubules resulting in the development of striations
Striated nephrogram Acute nephritis Acute obstructive uropathy
Acute extrarenal obstruction- Pathogenesis-disputed • Dense striae represent hyperconcentration of contrast in dilated collecting ducts that extend from inner cortex to tip of papillae in bundles (medullary rays) • Linear lucencies rather than densities are abnormal & are the result of reflux of nonopacified urine from PCS
Seen in- • Acute extrarenal obstruction • Acute bacterial nephritis • Acute pyelonephritis • Renal contusion • Autosomal recessive infantile polycystic kidney disease • Medullary cystic disease • Medullary sponge kidney
Patchy nephrogram Definition-inhomogeneous nephrogram consisting of patchy densities. Seen in- • Polyarteritis nodosa • Scleroderma • Necrotizing angiitis
Cortical rim nephrogram Def- Only the thin rim of peripheral cortex is opacified. • The opacified rim represents the peripheral cortex that is perfused by capsular collateral arteries • It is a reliable indicator of underperfusion of kidney Seen in- • Infarction of either entire or major portion of kidney 2. Renal vein thrombosis Cortical rim sign in segmental RA occlusion
Cortical rim sign must be distinguished from the rim sign seen in chronic obstructive nephropathy. • The opacification compressed atrophic renal parenchyma giving rim sign in chronic obstructive nephropathy is slower & less dense than that of contralateral side Rim sign of chronic obstructive uropathy
RETROGRADE PYELOURETEROGRAPHY • INDICATIONS: 1. Demonstration of the site, length,lower limit and if possible, the nature of an obstructive lesion. 2. Demonstration of the pelvicalyceal system after an unsatisfactory excretion urogram . Seldom necessary with modern imaging methods. • CONTRAINDICATIONS: Acute urinary tract infection • CONTRAST MEDIUM HOCM or LOCM 150-200, ie. Not too dense to obscure small lesions , 10ml. • EQUIPMENT Fluoroscopy unit
TECHNIQUE • In the OT The surgeon catheterises the ureter via a cystoscope and advances the ureteric catheter to the desired level . Contrast medium is injected under fluoroscopic control and spot films are exposed. • IN THE X RAY DEPTT 1.With ureteric catheter in situ, the patient is transferred from the operating theatre to the x-ray deptt. 2. Urine is aspirated and ,under fluoroscopic control, contrast medium is slowly injected. About 3-5ml are usually enough to fill the pelvis but the injection should be terminated before this if the pt complains of pain or fullness in the loin. 3.If there is PUJ obstruction, the contrast medium in the pelvis is aspirated. The films are examined and, if satisfactory, the catheter withdrawn, first to 10cm below the renal pelvis , and then to lie just above the ureteric orifice. About 2ml of contrast medium are injected at each of these levels and films taken