Download
1 / 37
370 likes | 543 Views
Urinary System. Kidneys: formation of urine -contains the functional unit for filtration = Nephron -production of urine, absorption of water and salts Ureters: transfer of urine from kidneys to bladder Urethra: transfer of urine from bladder to outside

E N D
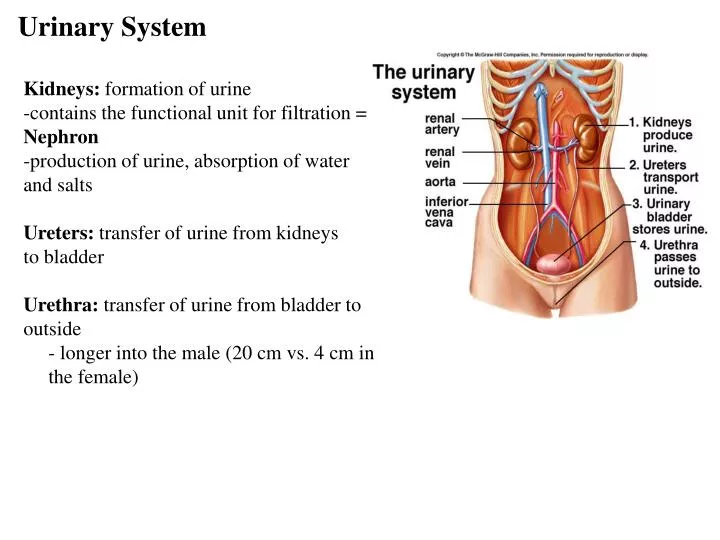
Urinary System Kidneys: formation of urine -contains the functional unit for filtration = Nephron -production of urine, absorption of water and salts Ureters: transfer of urine from kidneys to bladder Urethra: transfer of urine from bladder to outside - longer into the male (20 cm vs. 4 cm in the female)
Kidneys • 10-12 cm • retroperitoneal – behind the peritoneum • not part of the abdominal cavity • surrounded by three layers of tissue • 1. deepest layer = renal capsule – transparent sheet of dense irregular connective tissue • continuous with the outer coat of the ureter • 2. middle layer = adipose capsule • amass of fatty tissue surrounding the renal capsule • 3. outer layer = renal fascia • thin layer of dense irregular connective tissue that anchors the kidney to the abdominal wall • divided internally into an outer cortex and an inner medulla • medulla consists of 8 to 18 cone-shaped regions called renal pyramids • the wider base faces towards the cortex, the narrow region (renal papilla) projects down into a cup-like structure called a minor calyx • renal cortex is divided into an outer cortical zone and a deeper juxtamedullary zone • the cortex also extends down in between the pyramids to form the renal columns • renal lobe = renal pyramid + the overlying renal cortex + ½ the adjacent renal colum
Blood supply • supplied by a renal artery and drained by a renal vein(s) • kidney receives 20-25% of the resting cardiac output through the renal arteries (1200mL per minute) • renal artery divides into segmental arteries – supply segments of the kidney • the segmental arteries give off branches that pass through the renal columns – interlobar arteries • at the base on the renal pyramids – between the medulla and cortex – they are called arcuate arteries • divisions from the arcuate are called the interlobular arteries (pass between the renal lobes) • the afferent arterioles are derived from the interlobular arteries • afferent arteriole supplies one nephron and forms the glomerulus (capillary network) • drainage of the glomerulus is via the efferent arteriole • efferent arteriole forms the peritubular capillary network which surround the upper portions of the nephron • an extension of this network covers the lower portion of the nephron (loop of henle) – vasa recta • the peritubular capillaires form the interlobular veins – arcuate veins – interlobar veins – renal vein
The Nephron -about one million nephrons -kidneys filter 180 L fluid per day!!!! -each nephron is a renal corpuscle + renal tubules -renal corpuscle: filtering unit consisting of a tangled cluster of capillaries -> glomerulus + Bowman’s capsule -tubules: for reabsorption of water and ions leading to final urine volume and composition -PCT +Loop of Henle + DCT
Cortical Nephron • 80-85% of nephrons are cortical nephrons • Renal corpuscles are in outer cortex and loops of Henle lie mainly in cortex
Juxtamedullary Nephron • 15-20% of nephrons are juxtamedullary nephrons • Renal corpuscles close to medulla and long loops of Henle extend into deepest medulla enabling excretion of dilute or concentrated urine
Urinary System Function 1. Excretion of Metabolic Wastes: nitrogenous wastes -Urea: by-product of amino acid metabolism -produced when ammonia + carbon dioxide -Creatinine: produced by breakdown of creatine phosphate (high energy molecule reserve of muscles) -Uric acid: by-product of nucleotide breakdown -insoluble and ppts in the blood, concentrates in joints 2. Water-Salt balance of blood: reabsorption into blood from the descending Loop of Henle, from collecting duct -reclaim salt from the ascending portion of Loop of Henle -reclaim urea from bottom section of collecting duct -release of anti-diuretic hormone by pituitary: increase reabsorption of water 3. Acid-Base balance of blood: reabsorption of bicarbonate ions from urine in the nephron decreases levels in blood (decreases carbonic acid levels) -movement of hydrogen ions from blood into the nephron, combines with ammonia to form ammonium (NH4+)
4. Secretion of hormones: release of renin by kidneys which leads to release of aldosterone by adrenal glands (reabsorption of salts by kidneys) -release of erythropoietin by kidneys (stimulates RBC production) -activation of vitamin D produced by the skin
Water Balance -extracellular fluids: blood plasma, interstitial fluid, CSF, etc…. -intracellular fluids: cytosol -unique distribution of ions in ECF and ICF e.g. -intracellular fluids: higher potassium, phosphate, magnesium - lower sodium, chloride and bicarb ions than in extracellular fluid -of the 40 liters of water in the average male - 37% is ECF and 63% is ICF -so the kidney’s ability to modulate the composition of blood plasma can determine the composition of interstitial fluid and therefore ICF
Water Intake -average intake - 2.5 L (60% from drinking water, 30% from moist foods, 10% byproduct of metabolism) -regulation of intake - thirst center within the hypothalamus e.g. as body loses water - osmoreceptors within the thirst center detect increase in osmotic pressure within the ECF (increase as little as 1%) -drinking distends the stomach which inhibits signalling from the thirst center
Water output -loses through urine, feces and sweat plus respiration and skin evaporation -2.5 L of water must be lost for water balance -60% lost in urine, 6% in feces, 6% in sweat, 28% evaporation from skin and lungs -primary means of controlling output is through urine production -dehydration: ECF becomes concentrated - increase osmotic pressure - pressure increase detected by osmoreceptors in hypothalamus -posterior pituitary gland releases anti-diuretic hormone (ADH) -ADH causes distal convoluted tubule and collecting duct to increase water reabsorption -excess water intake: ECF less concentrated - decrease in O.P -osmoreceptors signal to the post. pituitary -P.P decreases ADH release -kidney/nephrons decrease water reabsorption
Renal physiology • comprised of filtration at the capsule (1) • reabsorption through the tubules (2) • direct secretion by the cells lining these tubules (3)
glomerulus: capillary tangle derived from afferent arterioles (into) and lead into efferent arterioles (out) • surrounded by a glomerular capsule (Bowman’s capsule) – single layer of epithelial cells • glomerular capsule: site of initial filtration and the first step in the formation of urine • consists of visceral and parietal layers • visceral layer consists of modified epithelial cells = podocytes • the podocytes wrap around the endothelial cells of the glomerular capillaries and forms the filtration membrane together with the endothelial cell wall • slits are covered with a slit membrane that permits the passage of small molecules such as water, vitamins, amino acids, wastes and small plasma proteins • space between the visceral and parietal layers = glomerular capsule • between the union of the afferent and efferent arterioles are mesangial cells that help regulate the rate of glomerular filtration
Renal Physiology • 1. Glomerular filtration • depends on three main pressures • 1. glomerular blood pressure (GBP) – BP in the glomerular capillaries (55 mmHg) • promotes filtration by forcing water and solutes through the filtration membrane • 2. caspsular hydrostatic pressure (CHP) – hydrostatic pressure exerted against the filtration membrane by fluid already in the bowman’s capsule • opposes filtration from the blood • 15 mm Hg • 3. blood collioid osmotic pressure (BCOP) – due to the presence of plasma proteins in the blood • opposes filtration from the blood • 30 mmHg • net filtration pressure (NFP) = GBP – CHP – BCOP = 10 mm Hg • loss of plasma proteins in the urine can cause edema (increased interstitial fluid) • damage to the glomerular capillaries can increase their permeabilty – loss of the larger plasma proteins • this increases the BCOP which draws larger amounts of water out of the blood and into the urine • but the BCOP decreases because we are losing these plasma proteins in the urine • the overall drop in BCOP causes water to leave the blood and enter the tissues systemically
Glomerular filtration rate • glomerular filtration rate (GFR) – amount of filtrate formed per minute (125 mL/min) • affected dramatically by NFP • adjusted by regulating: 1) blood flow into and out of the glomerulus and 2) the glomerular capillary surface area available for reabsorption • three mechanisms control GFR
GFR • 1. renal autoregulation – two mechanisms – myogenic mechanism and tubuloglomerular feedback • myogenic mechanism – increased blood volume can increased GFR • by the stretching of the afferent arterioles triggers the contraction of the smooth muscle lining these arterioles • tubulogomerular mechanism – feedback provided to the glomerulus from the renal tubules • increase in the fluid through the PCT, LH and DCT – less time to reabsorb materials • cells in these tubules induce vasoconstriction in the afferent arterioles • if GFR drops below normal – these cells stimulate the release of NO from the juxtaglomerular cells – vasodilation which increases blood flow and GFR • 2. neural regulation – sympathetic ANS fibers release norepinephrine which causes vasoconstriction of the smooth muscle in the afferent arteriole • 3. hormonal regulation • release of angiotensin II reduces GFR by inducing vasoconstriction • also release of atrial natriureic peptide (ANP – from the cardiac cells) increases GFP by increasing the surface area of the glomerulus
PCT and Loop of Henle • proximal convoluted tubule: first area of reabsorption into blood -> Loop of Henle -> distal convoluted tubule -> collecting duct -> union of ducts into ureter • cells of these tubules are also single epithelial layers – vary as either cuboidal (PCT and DCT, descending) or squamous (ascending LH) • PCT and DCT surrounded by the peritubular network of capillaries for reabsorption back into the blood, LH is covered with the vasa recta • PCT is the site of water reabsorption (PASSIVE) - associated with the ACTIVE reabsorption of sodium and potassium ions • active Na+ and K+ uptake by the blood from the PCT is by sodium pumps - sodium pumped from the PCT and chloride, bicarbonate and phosphate ions follow it - salt reabsorption • the active transport of ions into the blood plasma increases osmotic pressure within the blood • therefore water moves out of the PCT into the capillaries PASSIVELY! • PCT reabsorbs about 70% of filtered Na+, ions and water • the apical surface of the PCT epithelium forms microvilli which increases the surface area of this region
Loop of Henle • active transport of Na+ continues through the loop of Henle and DCT • descending loop of Henle is quite permeable to water but impermeable to solute movement – urine becomes hypertonic (increased ions within the urine, decreased water) • ascending loop is the opposite – permeable to salt (salt pumped out of the urine back • into the blood plasma) • the wall of the arterioles alongside the ascending portion of the LH contain modified smooth muscle cells = juxtaglomerular cells • regulate blood pressure within the kidneys
DCT and Collecting Duct • two types of cells found in the DCT and CD • principal cells – receptors for ADH and aldosterone • intercalated cells – play a role in the homeostasis of blood pH • DCT and collecting duct are impermeable to water !!!! • the DCT and CD become permeable upon action of hormones
Renal Physiology • Tubular reabsorption • tubule cells reabsorb about 99% of the filtered water and many of the solutes • principal materials reabsorbed – glucose, aminao acids, urea, Na+, K+, Ca+, Cl-, HCO3- and HPO4- • return to the blood through reabsorption into the peritubular capillary network and vasa recta • reabsorption = return to the blood • absorption = entrance of new materials into the blood (e.g. via digestive absorption) • reabsorption routes – one of two routes before re-entering the blood
Reabsorption Routes • Paracellular reabsorption • between adjacent tubule cells into the blood • 50% of reabsorbed materialmoves between cells bydiffusion in some parts oftubule • Transcellular reabsorption • material moves throughboth the apical and basalmembranes of the tubulecell by active transport
Renal Physiology • Tubular secretion • tubular cells also secrete other materials – wastes, drugs, excess ions into the urine • this also removes these materials from the blood
Reabsorption in the PCT • Na+ symporters help reabsorb materials from the tubular filtrate • Glucose, amino acids, lactic acid, water-soluble vitamins and other nutrients are completely reabsorbed in the first half of the proximal convoluted tubule • Intracellular sodium levels are kept low due to Na+/K+ pump Reabsorption of Nutrients
Reabsorption of Bicarbonate, Na+ & H+ Ions • Na+ antiporters reabsorb Na+ and secrete H+ • PCT cells produce the H+ & release bicarbonate ion to the peritubular capillaries • important buffering system • For every H+ secreted into the tubular fluid, one filtered bicarbonate eventually returns to the blood
Passive Reabsorption in the 2nd Half of PCT • Electrochemical gradients produced by symporters & antiporters causes passive reabsorption of other solutes • Cl-, K+, Ca+2, Mg+2 and urea passively diffuse into the peritubular capillaries • Promotes osmosis in PCT (especially permeable due to aquaporin-1 channels
Secretion of NH3 & NH4+ in PCT • Ammonia (NH3) is a poisonous waste product of protein deamination in the liver • most is converted to urea which is less toxic • Both ammonia & urea are filtered at the glomerus & secreted in the PCT • PCT cells deaminate glutamine in a process that generates both NH3 and new bicarbonate ion. • Bicarbonate diffuses into the bloodstream • during acidosis more bicarbonate is generated
Reabsorption in the Loop of Henle • Tubular fluid • PCT has reabsorbed 65% of the filtered water so chemical composition of tubular fluid in the loop of Henle is quite different from plasma • since many nutrients were reabsorbed as well, osmolarity of tubular fluid is close to that of blood
Symporters in the Loop of Henle • Thick limb of loop of Henle has Na+ K- Cl- symporters that reabsorb these ions • K+ leaks through K+ channels back into the tubular fluid leaving the interstitial fluid and blood with a negative charge • Cations passively move to the vasa recta
Reabsorption in the DCT • Removal of Na+ and Cl- continues in the DCT by means of Na+ Cl- symporters • Na+ and Cl- then reabsorbed into peritubular capillaries • DCT is major site where parathyroid hormone stimulates reabsorption of Ca+2 • DCT is not very permeable to water so it is not reabsorbed with little accompanying water
Reabsorption & Secretion in the Collecting Duct • By end of DCT, 95% of solutes & water have been reabsorbed and returned to the bloodstream • Cells in the collecting duct make the final adjustments • principal cells reabsorb Na+ and secrete K+ • intercalated cells reabsorb K+ & bicarbonate ions and secrete H+
Actions of the Principal Cells • Na+ enters principal cellsthrough leakage channels • Na+ pumps keep theconcentration of Na+ inthe cytosol low • Cells secrete variableamounts of K+, to adjustfor dietary changes in K+intake • down concentration gradient due to Na+/K+ pump • Aldosterone increases this Na+ reabsorption (and passive water reabsorption) & K+ secretion by principal cells by stimulating the synthesis of new pumps and channels.
Secretion of H+ and Absorption of Bicarbonate by Intercalated Cells • Proton pumps (H+ATPases) secrete H+ into tubular fluid • can secrete against a concentration gradient so urine can be 1000 times more acidic than blood • Cl-/HCO3- antiporters move bicarbonate ions into the blood • intercalated cells help regulate pH of body fluids • Urine is buffered by HPO4 2- and ammonia (secreted by cells of PCT), both of which combine irreversibly with H+ and are excreted
Production of Dilute or Concentrated Urine • Homeostasis of body fluids despite variable fluid intake • Kidneys regulate water loss in urine • ADH controls whether dilute or concentrated urine is formed • if lacking, urine contains high ratio of water to solutes • dilute urine – reabsorption of ions is unchanged (normal) but ADH decreases reabsorption of water
Summary • H2O Reabsorption • PCT---65% • loop---15% • DCT----10-15% • collecting duct--- 5-10% with ADH
Renin-Angiotensin-Aldosterone • when blood volume and BP drop – the walls of the afferent arterioles are stretched less – juxtaglomerular cells secrete renin into the blood (also stimulated by sympathetic stimulation) • in the blood renin cleaves angiotensinogen (made by hepatocytes) to form angiotensin I • the enzyme ACE (in the lung) – cleaves this even more to form angiotensin II • 1. decreases GFR by causing vasoconstriction of afferent arterioles • 2. enhances reabsorption of Na+, Cl+ and water in the PCT by stimulating the Na/H antiporter • 3. stimulates the release of aldosterone by the adrenal cortex – stimulates the principal cells of the DCT collecting ducts to reabsorb more Na and Cl and secrete more K into the blood • osmotic consequence of this causes an increased reabsorption of water
ADH and ANP • ADH – released by the posterior pituitary • regulated water reabsorption by increasing the permeability of the principal cells in the DCT to water • in the absence of ADH the principal cells of the DCT and CT have low permeability to water • within the principal cells are vesicles containing a protein called aquaporin-2 • ADH stimulates the insertion of aquaporin-2 into the apical membrane • water permeability increases • when the OP of the blood plasma increases (decreased water concentration ) via increased filtration – osmoreceptors in the hypothalamus detect this drop and stimulate the release of ADH • increased permability to water reintroduces water back into the blood and lower the OP of the blood plasma • ANP – inhibits the reabsorption of Na and water in the PCT and the collecting duct • also suppresses the secretion of aldosterone and ADH • increases the excretion of Na in the urine (natriuresis) and increase urine output (diuresis) which decreases blood volume and BP and inhibits its further release