Download
1 / 56
560 likes | 603 Views
Damage to the spine, pelvis. HEAD OF DEPARTMENT. PR OFESSOR Fishchenko Vladimir Alexandrovich. BASHINSKIY GENNADIY PETROVICH. Among spinal injuries most noteworthy damage to the vertebrae themselves. Early diagnosis of the spine is very important to provide the correct and timely fast aid.

E N D
HEAD OF DEPARTMENT PROFESSOR Fishchenko Vladimir Alexandrovich
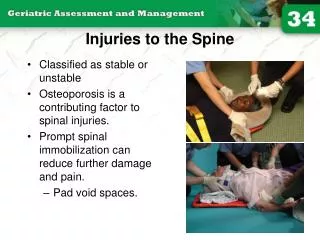
Among spinal injuries most noteworthy damage to the vertebrae themselves. Early diagnosis of the spine is very important to provide the correct and timely fast aid
Late diagnosis may cause worsening of spinal cord injury and quickly lead to secondary damage to the spinal cord and its roots
The cause of delayed diagnosis of spinal injuries is usually underestimating the severity of the damage. It should be remembered that the diagnosis of a back injury, ligament damage, etc. can be considered only after it is completely excluded the diagnosis damage of the vertebral body
nd its extension Damage to the vertebral bodies are more common in the indirect mechanism of injury: the axial load on the spine, sharp or excessive flexsion and its extension .
Sometimes there may be two or even three types of loads. For example, the combination of a sharp flexion and extension of the cervical spine when hit by a car, braking, etc.
In adults, the most damaged by the lower neck and upper chest vertebrae, the lower thoracic and upper lumbar vertebrae (the transition zone of one of the physiological curvature of the other).
Dislocation are more common in the cervical region, while in the thoracic and lumbar region we can see fractures and fracture- dislocation.
Damage to the vertebral bodies are divided into: stable and unstable. The instability called those injuries for which there is a tendency to shift the vertebrae, which is observed in posterior ligamentous complex (interspinous, supraspinous, yellow ligaments and intervertebral joints).
Rear ligamentous complex also damaged at fracture-dislocations of the vertebrae, with wedge compression by more than half the height of the vertebral body
Stable fractures are rarely associated with the pressure of the contents of the spinal canal, and in unstable injuries is always a dangerof such a compression
It is also unstable so-called flexion - rotation fracture. The most common fractures of the vertebrae - wedge compression and the abruption anterosuperior and anteroinferior angle - are stable fractures.
classification of fractures of the spine in the degree of compression • 1 degree -height of the vertebral body is reduced to one-third2 Degree - half3 Degree - more than half
Diagnosis of vertebral fractures and dislocations • The most common complaint of patients early after injury is a pain in the injured spine, which spans 2-3 vertebrae. Pain may be local or radicular
When viewed from the back should first pay attention to changes in the physiological curvature of the spine. True hump is rare, but the decrease of lumbar lordosis or increase thoracic kyphosis is often observed
In fractures the lumbar vertebrae can be a pain in the abdomen and some muscle tension anterior abdominal wall. This is due to the presence of retroperitoneal hematoma accompanying fracture.
The presence of retroperitoneal hematoma, irritation or damage to the solar plexus and border symptomatic trunk carried to the emergence of " the clinic false "acute abdomen", which can be so severe that sometimes have to resort to a diagnostic laparoscopy or laparotomy.
For the differential diagnosis between the clinic false "acute abdomen", abdominal syndrome in fractures of the lumbar vertebrae and damage to the organs of the abdominal cavity, you can use vertebra anesthesia by Shnek.
Anesthesia performed with the patient on his side. 12-14 cm long needle is introduced at 6 cm away from the spinous processes of the lumbar vertebrae and broken promote vertebral body at an angle of 35 degrees to the plane of the back. At a depth of 5-8 cm needle usually rests on the transverse process. Surpassing its top, the needle move further the midline.
The movement of the needle precede the introduction of a 0.5% solution of novocaine. At a depth of 8-12 cm needle rests in the body of broken vertebra. Confirmation of this will leak out of the needle novocaine stained with blood. Here are administered 10 ml of a 1% solution of novocaine. The needle is removed.
If after a few minutes of anesthesia by Shnek you can noticeregression of symptoms of "acute abdomen", you can think of that syndrome is caused by a fractured vertebra.
Fairly constant symptom of spinal injury is increased pain in the back straight when lifting the leg with the supine position. But this symptom is characteristic not only of vertebral fractures in the lumbar region, but also for any back injuries in general, including bruises, sprains and back muscles etc
In order that would differentiate a fracture of the body of the lumbar or lower thoracic vertebrae from the back of soft tissue injury and fractures of the transverse processes, there should be palpated spinous processes while lifting straight feet from a lying position on the back (a symptom of Silin).
The axial load on the vertebra is allowed only with the patient lying in a light tapping on the heels or the pressure on the head. Rough axial load on the spine and determination of volume of movement especially in the upright position of the patient, are not allowed.
Conservative treatment:Method of single repositioning followed by the imposition corset;Functional method;The method of gradual repositioning followed by the imposition corset
One-step repositioning is carried out at a safe anesthetic. The simplest method is by Boehler when Interspinous span over a broken vertebra at a depth of 2-4 cm injected 20 ml of 0.5% solution of novocaine. Better pain relief reaches properly performed anesthesia by Shnek, but it is technically difficult and should not be performed because of the budding traumatologist possible complications. Local anesthesia supplemented subcutaneous analgesics
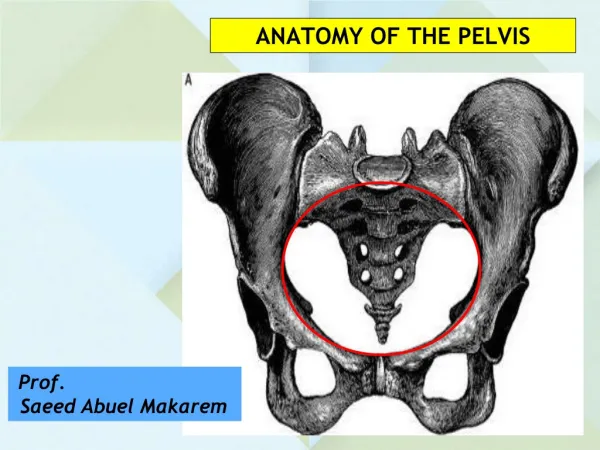
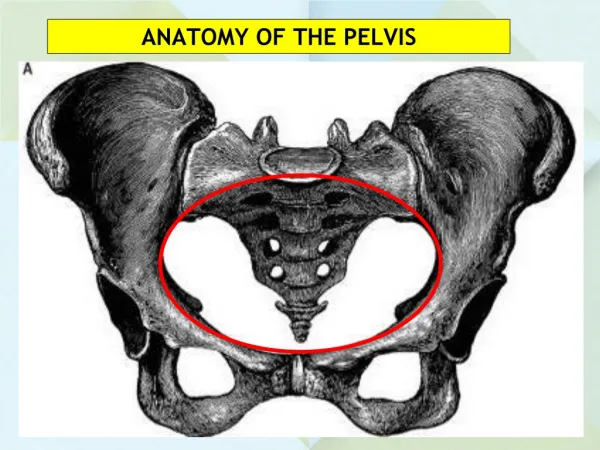
Fractures of the bones of the pelvis • Damage to the bones of the pelvis is 4-7% of all fractures and are a group of serious injury. Damage to the pelvis may be accompanied by the most severe shock caused by irritation of the rich reflexogenic zones and massive bleeding into the tissues of the spongy bone (more than 2 liters)
One of the functions of the pelvis - the transfer of the trunk load on the lower limbs (supporting the pelvis) is due to the integrity of the pelvic ring. Pelvic ring formed by the sacrum, the body of the ilium, pubic and ischial bones (excluding the ischial tuberosity), pubic and sacroiliac joint.
A. Boundary value fractures • This damages the pelvic bones are not involved in the formation of the pelvic ring. This group includes broken spinal process, tuber of ischium, coccyx, transverse fracture of the sacrum below the sacroiliac joint, fractures of the ilium
Marginal fractures • The mechanism of injury is the direct Fractures of the iliac wing, after brief compression of the pelvis. Fractures of the anterior spine may be during heavy muscle tension. Fractures of the sacrum below the sacroiliac joint and coccyx occurs when falling on the buttocks
By tearing the anterior spine, tenderness in the area of separation, local swelling, a false impression of shortening due to downward and outward displacement of the fragment. Symptom-Lozinski (reverse) - when you try to bend the thigh during a step forward there is a sharp pain in the area of the fracture due to muscle tension clip-on to the spine. The movement kicked back is significantly less pain, a patient walks back
B. Fractures of the pelvic ring without breaking its continuity • This bone fractures, forming the pelvic ring. The strength of the pelvic ring is reduced, but the reference is stored as the two halves of the pelvis are connected with the sacrum, both directly and through the other half
These injuries include:One or bilateral fractures same branch pubic bone;Single or bilateral fractures of the ischial bones;Fracture of one of the branches of the pubic bone on one side and the other of the ischium.
Fractures of the pelvic ring without breaking its continuity • The mechanism of injury-line. Complaints: pain in the pubic area, in the crotch on the side of injury. Symptom-Gabai when turning from back to side-step the patient maintains a damaged side of the pelvis lower legs or feet healthy side, turning from a lateral position on the back of the patient keeps this fixed position of both legs. Symptom "stuck heel" - the patient can not take his foot from the support line, but keeps the limb elevated themselves
B. Damage to the violation of the continuity of the pelvic ring • In such injuries each half of the pelvis is soldered to the sacrum with only one side. Greatly disturbed the support function of the pelvis.Among these injuries :Vertical fracture of the sacrum, or fracture of the lateral mass of the sacrum;Rupture of the sacroiliac joint
Vertical fracture of the ilium;. Fracture of both branches of the frontal bone on one or both sides;. Fracture of the pubic and ischial bones on one or both sides (fracture of the "butterfly");. Rupture symphysis;
Damage to the solution of continuity with simultaneous front and back half-rings (like Malgeniya). With this type of injury is completely lost connection half of the pelvis with sacrum. The support function of the pelvis and half lost. Half of the pelvis that is not related to the spine (sacrum to), under the thrust of the back muscles and stomach moves up.
MAY BEBilateral fracture type Malgenya when and the front and back D-rings are damaged on both sides;Unilateral or vertical, fracture type Malgenya - fracture of front and back half-rings on the one hand;Oblique or diagonal fracture Melgenya - the front half ring broken one, and the rear - on the other side;
Fractures of the acetabulum: • rupture of the sacroiliac joint and symphysis; • The combination of the symphysis fracture with fracture back D-rings, or a combination of rupture sacroiliac joint with a fracture of the front D-rings
Fractures of the acetabulum: Fracture edge of the acetabulum,(with a dislocated hip, often caudineural)Fracture of the bottom of the acetabulum,(with central dislocation of the hip)
The mechanism of injury, the lateral compression of the pelvis in the trochanter. The clinic is smoothed, X-ray examination is mandatory. Treatment-conservative-skeletal traction. Acetabular fractures with central dislocation of the hip-skeletal traction is applied along the axis of the thigh and the side of the greater trochanter