Download

1 / 43
431 likes | 625 Views
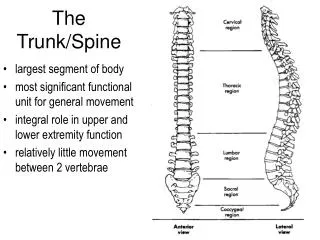
The Spine. Anatomy. The movable vertebrae are separated into 3 divisions: Cervical (7), Thoracic (12), Lumbar (5) Each vertebra consist of a neural arch through which the spinal cord passes, and have several projecting processes that serve as attachments for muscles and ligaments. Anatomy.

E N D
Anatomy • The movable vertebrae are separated into 3 divisions: Cervical (7), Thoracic (12), Lumbar (5) • Each vertebra consist of a neural arch through which the spinal cord passes, and have several projecting processes that serve as attachments for muscles and ligaments.
Anatomy • Each vertebra has a spinous and transverse process, except the atlas and axis. • All vertebrae have an articular process • Spine consists of a normal cervical, thoracic, and lumbar curve.
Cervical Spine • 7 vertebrae • First two are the Atlas & Axis • Atlas – functionally supports head, allows for flexion and extension, and some lateral movement • Axis – allows the atlas to rotate on it, has a toothlike projection (odontoid process) that fits into the ring of the atlas. • The cervical spine is very mobile due to flattened, oblique facing of its articular facets and to the horizontal positioning of the spinous processes.
Thoracic Spine • 12 vertebrae • Long transverse processes, prominent thin spinous processes • 1-10 have articular facets for the ribs to articulate
Lumbar Spine • 5 vertebrae • Large and thick, with large spinous and transverse processes. • Movement is present in all lumbar vertebrae, but less flexion than extension.
Sacrum • In the adult, the sacrum is the fusion of 5 vertebrae, and in conjunction with the hips, it forms the pelvis. • The sacrum articulates with the illium to form the sacroiliac joint.
Coccyx • Tailbone • Most inferior portion of the vertebral column • Made up by 4 or more fused vertebrae. • The gluteus maximus attaches to the coccyx
Intervetebral Disks • Between each vertebrae lie fibrocartilaginous disks. • Disks serve as shock absorbers for the spine.
Ligaments • 3 major ligaments • Anterior longitudinal, Posterior Longitudinal, & Supraspinous • Anterior – strong wide band that runs full length of the anterior surface of the spinal column. • Posterior – contained within the canal and runs the full length of the posterior portion of the vertebrae • Supraspinous – connect one lamina to another.
Movements of the Spine • Flexion • Extension • Lateral Flexion • Rotation
Muscles of the Cervical Spine • Sternocleidomastoid: Flexion • Scalene: Flexion • Trapezius: Extension • Semispinalis Capitis: Extension • Spenius Capitis: Extension • Spenius Cervicis: Exetnsion
Muscles of the Spine • Classified as superficial or deep • Erector Spinae make up the superficial; paired group that make up three bands. Help extend the spine • Deep muscles extend and rotate the spine • Flexion involves lengthening the back muscles and contraction of the abdominal muscles. • Rotation involves the external and internal obliques • Lateral Flexion is produced by the obliques, latissimus dorsi, iliopsoas, abdominals, and quadratus lumborum.
Spinal Nerves • 31 pair of spinal nerves • 8 cervical, 12 thoracic, 5 lumbar, 5 sacral, 1 coccygeal • Each has an anterior and posterior root. • There are 5 nerve plexuses: cervical, brachial, lumbar, sacral, coccygeal
Postural Deviations • Kyphosis: increased thoracic curve, rounded shoulder appearance • Forward head: extended cervical spine, weak long neck flexors • Flatback: decreased lumbar curve, and increased posterior pelvic tilt and hip flexion • Swayback: anterior shift of pelvis. Decrease in lordosis, flexion of thorax • Lordosis: increased lumbar curve • Scoliosis: lateral curve of the spine
Neck & Back Injuries • Cervical Fracture – Most common in the 4th, 5th, and 6th vertebrae. Caused by axial loading with flexion • Signs & Symptoms: Pt tenderness, restricted ROM, muscle spasm, pain in the chest, extremities, & cervical spine. Numbness in trunk or limbs, weakness or paralysis in the limbs or trunk, loss of bladder or bowel control. • Management: Medical emergency, back boarding procedure
Neck & Back Injuries • Cervical Dislocations • Result from violent flexion and rotation of the head • Signs & Symptoms: Many of the same symptoms as a fracture. A unilateral dislocation will cause the neck to be tilted toward the dislocated side • Management: Medical emergency, back boarding procedure
Neck & Back Injuries • Neck Strain & Sprains • Sudden movement or forced flexion, extension, or rotation • Signs & Symptoms: Localized pain, pt tenderness, limited ROM, & muscle guarding. Symptoms for a sprain will last longer and there may be tenderness over the transverse and spinous processes. • Management: RICE, a sprain may need further evaluation by a physician to rule out fracture, dislocation, or disk injury.
Neck & Back Injuries • Cervical Cord and Nerve Root Injuries • Laceration • Hemorrhage • Contusion • Spinal Cord Shock – mild contusion to the spinal cord causing temporary weakness, numbness, or tingling in the arms or legs.
Neck & Back Injuries • Cervical Stenosis • Narrowing of the spinal canal in the cervical spine • Signs & Symptoms: Transient quadriplegia, burning, tingling, or motor weakness in extremities. Recovery in about 10-15 minutes. • Management: Advise athlete of potential risks, and discourage from participating.
Neck & Back Injuries • Brachial Plexus Neurapraxia (Burner) • Transient neurapraxia from stretching or compressing the brachial plexus
Neck & Back Injuries • Lumbar Strains & Sprains • Sudden extension contraction on an overloaded, unprepared, or underdeveloped spine, usually with trunk rotation • Signs & Symptoms: Rule out fracture, pain with active extension & passive flexion, localized pain with a sprain • Management: RICE, progress to stretching and strengthening
Neck & Back Injuries • Herniated Lumbar Disk • Stresses from trauma and/or faulty body mechanics • Signs & Symptoms: Localized pain that radiates unilaterally in a dermatomal pattern. Pain is generally worse in the AM. Forward bending increases pain, posterior bending decreases pain. Straight leg raise to 30degrees increases pain. • Management: Modalities to treat pain, teach posture and strengthening exercises. Symptoms may resolve with time, surgery may be required if there are signs of nerve damage.
Neck & Back Injuries • Spondylolysis & Spondylolisthesis • Degeneration of the vertebrae, defect in the pars interarticularis of the articular processes of the vertebrae. • Signs & Symptoms: Persistent aching pain or stiffness across back, increased pain after exercise. Decreased strength and hesitant to move into flexion. May have some pt tenderness and hypermobility. • Management: Modalities, rest, strengthening, may discuss options to avoid vigorous activities.
Neck & Back Injuries • Sacroilliac Sprain • Twisting with feet planted, miss-stepping, bending with the knees locked, falling backwards, or stumbling forwards • Signs & Symptoms: Pt tenderness, ASIS or PSIS asymmetry, leg-length difference, increased pain with side bending and leg raise past 45degrees. • Management: Modalities, strengthening, mobilization of SI joint.
Neck & Back Injuries • Coccyx Injuries • Occur from direct impact, falling, or sitting forcefully. • Signs & Symptoms: Persistent pain should be x-rayed. • Management: Ring seat, padding once injury has healed.
Special Tests • Standing – observe gait, note symmetry of malleoli, trochanters, ASIS, PSIS, illiac crests, and popliteal crease. Flexion & extension • Sitting – Trunk rotation, hip external & internal rotation. • Supine – straight leg raise 30 (hip or inflamed nerve), 30-60 (sciatic nerve), 70-90 degrees (SI joint) • Prone – press up, if pain radiates it may indicate a herniated disk.
Special Tests • Bowstring – leg on affected side if lifted until pain is felt, then the knee is flexed until pain is relieved. Sciatic nerve irritation. • FABER – indicates problem with SI joint. • Sacroilliac compression/distraction - indicates problem with SI joint. • Neurological – dermatomes, reflexes • Cervical compression – Axial compression, compressing cervical spine, indicating which nerve is injured.