Download
1 / 23
240 likes | 283 Views
Specific Uveitis Syndromes. Behect’s Disease Vogot-Kaynagi–Hadra Syndrome Endophthalmitis & panophthalmitis Sympathetic Ophthalmitis. (1) Behcet’s Disease. ● Systemic features: ►It is characterized by a Traid of: Recurrent mouth ulcers, Genital ulcers, and Uveitis.

E N D
Specific Uveitis Syndromes • Behect’s Disease • Vogot-Kaynagi–Hadra Syndrome • Endophthalmitis & panophthalmitis • Sympathetic Ophthalmitis
(1) Behcet’s Disease ● Systemic features: ►It is characterized by a Traid of: • Recurrent mouth ulcers, • Genital ulcers, and • Uveitis.
Behcet's disease. Top left: ulcer of buccal mucosa; top right: tongue ulcer; Bottom left: genital ulceration; Bottom right: leg edema 2ry to severe thrombophlebitis
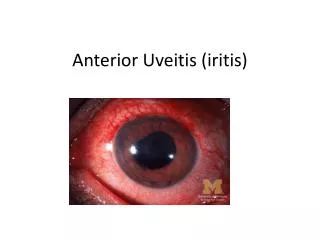
● Ocular features: (a) Anterior uveitis: recurrent, non-granulomatous, and may be associated with hypopyon. Acute iridocyclitis with hypopyon associated with Behcet's disease.
(b)Posterior segment involvement • Diffuse vascular leakage associated with retinal edema and CME. 2. Periphlebitis which may cause venous occlusion and secondary retinal NV. 3. Retinitis in the form of transient white necrotic infiltrates. 4. Acute massive retinal exudation leading to necrosis and atrophy.
(2) Vogot-Kaynagi–Hadra Syndrome • V-K-H syndrome is an idiopathic, multisystem disorder which typically affects pigmented individuals. • In clinical practice, V-K-H syndrome can be subdivided into: • V-K syndrome characterized mainly by skin changes and anterior uveitis; and • Harada's disease characterized mainly by neurological features and exudative RD.
● Systemic features: (a) Cutaneous features include: 1. Vitiligo (patches of skin depigmentation) 2. Alopecia (loss of hair) 3. Poliosis (whitening of eyelashes). Vitiligo in VKH syndrome
(b) Neurological features include: 1. Headache and neck stiffness 2. Encephalopathy 3. Auditory features(tinnitus, vertigo, and deafness). 4. CSF lymphocytosis
● Ocular features: 1. Chronic granulomatous anterior uveitis (iridocyclitis) 2. Multifocal Choroiditis 3. Exudative RD in harada's disease. Exudative RD in Harada's disease
(3) Endophthalmitis • Definition: Acute suppurative inflammation inside the globe. • The outer coat of the globe (cornea & sclera) and Tenon’s capsule are not involved in endophthalmitis.
Aetiology: • Exogenous infection:- • Perforaled corneal ulcer • Penetrating trauma • Postoperative infection b. Endogenus:- Septicaemia pyaemia.
Clinical picture: a. Symptoms: • severe visual loss (up to NPL) according to severity. • constitutional symptoms as fever, malaise. • severe pain and headache.
b.Signs: • Eyelids:Lid edema and redness. • Conjunctiva: conjunctival edema (chemosis) and injection • Cornea: corneal haziness (edema) and KPs. • Anterior chamber: Hypopyon. • Fundus:yellow reflex due to pus in the vitreous. • No proptosis or ocular motility limitation.
Treatment of endophthalmitis: • Start treatment as soon as possible even before the results of the culture sensitivity samples from aqueous tap and vitreous tap. A. Early cases: a. Medical: Antibiotics: Broad-spectrum antibiotics are given by all routes: • Topically • Subconjunctivally • Systemically (iv.) b. Surgical: - Intravitreal injections - Pars-plana victrectomy. Indications: 1. To remove the infected vitceous . 2. To make antibiotic treatment more effective . 3. To get samples for culture and sensitivity.
B. Late cases: evisceration (not enucleation) N.B. Enucleation is contraindicated in endophthalmitis because it opens the sheaths of the optic nerve spread of infection (along the subarachnoid space) to the brain meningitis
(4) Panophthalmitis • Definition: Acute suppurative inflammation which involves all the ocular-coats including the outer coat “cornea, sclera” , Tenon’s capsule and orbital cellular tissues. • Aetiology: • As in endophthalmitis but exogenous infection is the usual cause (more common than endogenous infections).
Clinical picture : • Symptoms: As endophthalmitis but severer. • Signs: As endophthalmitis + 1. ring abscess in the cornea. 2. Signs of Tenon’s capsule involvement: a. proptosis. b. limitaion of extraocular motility. • N.B. No proptosis nor limitation of ocular motility in endophthalmitis because the Tenon’s capsule is Not involved. • Complications: • atrophia bulbi. • spread of infection: a. Orbital cellulitis b. Cavernous sinus thrombosis. c. Meningitis.
Differential Diagnosis: 1. Endophthalmitis 2. Orbital Cellulitis 3. Cavernous sinus thrombosis. • Treatment: • Evisceration (not enucleation).
(5)Sympathetic ophthamitis • Definition: • Is a serious bilateral inflammation of uveal tract in a normal eye (sympathising) As a response to. • inflammation in the other injuried eye “with penetrating injury” (exciting eye). Sympathising Exciting eye
Aetiology: • It usually follows penetrating injuries of the globe especially in the ciliary body region (dangerous area) with: - Incarceration of iris, CB, or lens capsule in the wound or - Retained IQFB.
Clinical picture (Bilateral) A. Exciting eye: • evidence of trauma or ocular surgery • Clinical picture of iridocyclitis which has not subsided for 3-4 weeks. B. Sympathising eye: • Onset: 4-8 weeks after injury or surgery (rarely up to years) • Prodromal symptoms: - photophobia and lacrimation. - disturbed near vision due to affection of accommodation. • Signs: of iridocyclitis of varying severity • Compilications: • 1. choroiditis & RD • 2. Complicated cataract • 3. secondary glaucoma • 4. atrophia bulbi.
Treatment: • Prophylactic treatment: • Proper treatment of ocular wounds with removal of IQFBs, • excision of prolapsed uvea and preventing incarceration of tissues in the wound. • Enucleation: of badly damaged globe with no hope for vision. B. Curative • (if prodromal symptoms appeared in the sympathising eye): • For the injured eye: a. Enucleation if the eye is seriously damaged with no hope for useful vision, this will stop the inflammation in the sympathising eye unless the inflammation started, then it will decrease but not stop it.B: Treatment of iridocyclitis aggressively if this eye hasa good vision especially if it is the better eye by topical and systemic steroids and cytotoxic drugs. 2. For the sympathising eye: • Treatment of iridocylitis (as in the injuried eye).