Download
1 / 46
460 likes | 595 Views
PULMONARY REABILITATION. A. CHABBOU MD MP Journées Scientifiques: SOUSSE LE 25 FEVRIER 2006. PULMONARY REABILITATION Rationel. The limitations of the patient with COPD Deconditioning ) impact on skeletal muscle Systemic manifestations ) and cardiovscular system

E N D
PULMONARY REABILITATION A. CHABBOU MD MP Journées Scientifiques: SOUSSE LE 25 FEVRIER 2006
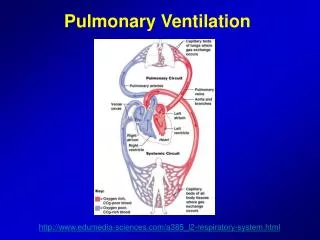
PULMONARY REABILITATIONRationel The limitations of the patient with COPD • Deconditioning ) impact on skeletal muscle • Systemic manifestations ) and cardiovscular system muscle dysfunctionEXERCISE LIMITATIONS inability to increase oxygen delivery to the peripheral muscle Pulmonary hypertension Constraints on lung mechanics During exercice (dynamic hyperinflamation and flow limitation) gaz exchange inefficiency in the lungs Cardio vascularPulmonary limitations Limitation Limitations are - cardiovascular - pulmonary - and skeletel muscle
PULMONARY REABILITATIONSkeletal muscle dysfunction : - déterminant factors - complementary mechanisms : 1- muscle strength exercise traning 2- muscle endurance 3- impaired muscle oxidative capacity - activity of the enzymes : citrate synthase hydrooxy acetyl COA deshydrogenase 4- a shift toward a glycolytic fiber type distribution (low fraction of type I fibers)* skeletal muscle endurance fatigability exercise training Lowering of the lactate threshold ventilatory requirements during exercise
PULMONARY REABILITATIONSkeletal muscle dysfunction* Proportion of type-IIA fibres % 29.4¡12.1 34.8¡11.9 Proportion of type-IIXfibres % 27.2¡12.345.8¡18.9** CSA of type-IIX fibres mm2 4248¡1300 2566¡1137** P<0.001 Myopathological features in skeletal muscle of patients with chronic obstructive pulmonary disease H.R. Gosker*, B. Kubat#, G. Schaart}, G.J. van der Vussez, E.F.M. Wouters*, A.M.W.J. Schols*
PULMONARY REABILITATIONComplementary mecanisms 1- The sedentary life style of COPD patients skeletal muscle atrophy at 2 levels : • The whole muscle level • The myocyte level With indirectly : the loss in fat-free mass 2- Systemic inflammation**: recent studies have underlined the importance of systemic inflammation as a mechanism for developement of muscle weakness, especially during severe exacerbations of COPD • Circulating levels of IL8 : are significantly correlated with muscle weakness • Weight loss, especially fat-free masshas been associated with systemic inflammation • levels of skeletal muscle apoptosis were observed in patients presenting with weight loss • Oxidative stress is another factor related to the process of muscle wasting.** • Patients with COPD are exposed to levels of oxidative stress : • when stable • and during exacerbations
PULMONARY REABILITATIONSystemic inflammation Nitrite and nitrate levels in patients with chronic obstructive pulmonary disease ( ) and control subjects ( ). *: p<0.05; **: p<0.01. Skeletal muscle inflammation and nitric oxide in patients with COPD M. Montes de Oca1, S. H. Torres2, J. De Sanctis3, A. Mata1, N. Hernández2 and C. Tálamo1 Eur Respir J 2005; 26:390-397
PULMONARY REABILITATIONSystemic inflammation Endothelial constitutive nitric oxide synthases (eNOS), inducible isoform nitric oxide synthases (iNOS) and nitrotyrosine levels in patients with chronic obstructive pulmonary disease ( ) and control subjects ( ). ***: p<0.001.
PULMONARY REABILITATIONSystemic inflammation Tumour necrosis factor (TNF)- levels in patients with chronic obstructive pulmonary disease ( ) and control subjects ( ). #: p<0.0001.
Variables Nitrites µmol·mg–1 protein 11.4±2.0 13.6±3.1 NS Low weight COPD Nitrates µmol·mg–1 protein 19.5±2.2 24.5±2.9 NS Total µmol·mg–1 protein 30.9±3,5 34.3±2.8 NS Nitrotyrosine ng·mg–1 protein 24.5±6.9 25.2±0.1 NS iNOS ng·mg–1 protein 27.1±7.6 36.6±9.4 NS eNOS ng·mg–1 protein 32.2±6.2 31.9±3.1 NS nNOS ng·mg–1 protein 85.3±18.4 101.7±23.1 NS TNF- pg·mg–1 protein 201±93 267±207 NS CD163 ng·mg–1 protein 6.4±0.7 6.8±2.7 NS CD154 ng·mg–1 protein 14.3±5.9 17.6±8.5 NS Table. — Skeletal muscle levels of inflammatory markers in low and normal weight chronic obstructive pulmonary disease(COPD) Normal weight COPD P-value
PULMONARY REABILITATIONSystemic inflammation Transversal section of the vastus lateralis part of quadriceps muscle. Immunohistochemical reaction with anti-CD68, clone MB11. a) Control subject, male aged 68 yrs. The black dots are muscle fibres and endothelial cell nuclei. b) Chronic obstructive pulmonary disease patient, male aged 68 yrs. The black stain represents macrophages infiltrate. Scale bar = 50 µm.
Oblique section of vastus lateralis part of quadriceps muscle in a 70-yr old female chronic obstructive pulmonary disease (COPD) patient. b) Longitudinal section of vastus lateralis part of quadriceps muscle in a 69-yr-old female COPD patient. Arrows show prolongations of macrophage surrounding capillary. M: macrophage; NM: nucleus of macrophage; F: muscle fibres; NF: nucleus of muscle fibre; C: capillary; NE: nucleus of capillary endothelial cell; P: pericyte. Scale bars = 1 µm.
PULMONARY REABILITATION Exercice intolerance : Multifactorial Impairment of lung mechanics Altered gaz exchange Impairment of respiratory muscles Cardiac dysfuntion Deconditioning Poor nutritional status Psychological problems
PULMONARY REABILITATION Disease Deficiency Incapacity Handicap COPD Aw obstruction dyspnea prostration COPD Bronchodilatation Tolerance Move PULMONARY REHABILITATION
PULMONARY REABILITATIONGoals - General :Improve physical and psychological or emotional functioning of patients in interaction with theire environment - Specific : - Reduce symptoms - Improve activity and daily function QOL - Restore the highest level of independant function (in every day activities) - Enhance knowledge of the disease - Improve self-management Non pulmonary problems Not addressed by medical therapy
PULMONARY REABILITATIONComponents of the rehabilitation program 1- Optimal medical treatment 2- Smoking cessation 3- Exercise training 4- Breathing retraining 5- Chest physiotherapy 6- Education 7- Psychological aspects and support 8- Nutritional therapy 9- Nursing care 10- Miscellaneous
PULMONARY REABILITATIONExercise Training Limitations inability toO2 delivery to muscles Needs Exercise Training inefficiency of Adapted to the gaz exchange Individual lung mechanics hyper inflation flow limitation Training programs pulmonary that stimulates hypertention cardiovascular and during exercise skeletal muscle muscle dysfunction
PULMONARY REABILITATIONExercise training - Lower extremity training : lower limbs exercise - Upper extremity training : arms exercise - Respiratory muscles training : respiratory muscles exercise
PULMONARY REABILITATIONExercise training Modalities Inpatient setting Out patient setting Community based setting Home based setting Inpatient setting - transdisciplinary team - favorable environnement and climate - Patient entire disponibility - 24 houres prolonged and tight management for weak patients
PULMONARY REABILITATIONExercise training 1- Methods • Cycle ergometer • Walking (Treadmill) Better physiological benefit when exercise above a «critical level of intensity» 2- Patients selection* Preliminary exercise test Resting respiratory function measurements (poor correlation) 3- Type of exercise : - intensity** - endurance 4- Duration : No ideal duration established 8 weeks : common duration*** 5- Results: Physiological change : **** blood lactate ventilation endurance After high work rate training programs
PULMONARY REABILITATIONExercise training Duration of programs Key Goal change the patient’s behavion from a sedentary toward a more active life style Measurable physiological changes : weeks behavioral changes months Longer duration Better long term effect > 8 weeks 6 months > 3 mouths
PULMONARY REABILITATIONResults • Increase in maximal exercise performance • Physiologic adaptations in peripheral muscles • Improve of cardiac function • Reduction in ventilation and lactate levels at identical exercise work rates
PULMONARY REABILITATIONExercise training Upper extremity Training - Improve arm muscles function - Does not improve exercise tolerance - Does not improve QOL
PULMONARY REABILITATIONExercise training Outcome measures : exercise testing • COPD patients mean age : 60 years • Most COPD patients are past smokers • COPD patients are at risk of other tobaco-related diseases : - ischemic cardiac diseases, arteriel HT, cardiac arrhythmias • Stress test for coronary disease : • 1 death/5000 • 1 major complication/1000 • Exercise testing in COPD patients : 1/3 arterial blood desaturation (SaO2 < 89 %) not predicted by rest spirometry nor CO diffusing capacity • Need of a preliminary exercise test
PULMONARY REABILITATIONExercise training Outcome measures: exercise testings Types of exercise tests 1- Submaximal exercise tests • cycle or treadmill • at a constant fraction of maximal work rate > 60 % of the peak V 02 • at low intensity, below to the lactic acidosis threshold • Measures exercise endurance • Measurements : endurance time, heart rate, respiratory rate, blood pressure, ECG, SaO2, exhaled gazes, inspiratory capacity
Exercise trainingOut come measures : exercise testing 2- Six minute walk test • Walks at his own pace • Simple, well tolerated and relevant to daily activites • But varies upon encouragement and coaching and should be standardized 3- Shuttle walk test • Walk up and down a 10 m distance with increasing speeds dictated by a beep • Measures more exercise capacity than endurance • But self pacing is eliminated • Reproductible and correlates well with VO2 peak during increamental treadmill exercise ( r= 0,88)
Exercise trainingOutcome measures : exercise testing Type of exercise tests 4- Incremental exercise tests • bicycle or treadmill • Measurements : Heart rate, respiratory rate, blood pressure, ECG, SaO2, dyspnea, leg fatigue, minute ventilation, oxygen consumption, CO2 production, anaerobic threshold and dead space • Equipment problems : • Cost of the test : 30 • Cost of equipement/test : 10
PULMONARY REABILITATION Level of Handicap Assessement Measures Deficiencies Respiration FEV1 • A Obstruction FRC • P.Elasticity IC • Gaz exchange DLCO PaO2, PaCO2, SaO2 Muscle • Respiratory MIP • Limbs and arms MEP Incapacity Dyspnea - Questionaires - Walk test 6 min Exercise - Endurance test - Exercise fonctional tests Disadvantage (handicap) QOL questionaires Life socio-professional
PULMONARY REABILITATIONExercise Training Specific strategies to increase training intensity Neuromuscular electrical stimulation (NES) Specific muscle groups of lower limbs are activated with low-intensity electrical current 2 trials of transcutaneous neuromuscular electrical stimulation of lower limbs in severe muscle weakness in stable patients - significant - muscle strength - exercise capacity 1 study : faster functionnal recovery in patients with respiratory failure under mechanical ventilation, bed bound for > 30 days. Zanotti E, Felicetti G, Maini M, Fracchia C. Peripheral muscle strength training in bed-bound patients with COPD receiving mechanical ventilation : effect of electrical stimulaiton. Chest 2003;124 : 292-296 NES is safe and can be conducted at home Neder JA, Sword D, Ward SA, Mackay E, Cochrane LM, Clark CJ. Home based neuromuacular electrial stimulation as pulmonary rehabilitation in chronic obstructuve pulmonary disease. Troosters et al
PULMONARY REABILITATIONExercise Training Specific strategies to increase training intensity Breathing exercises • Diaphragmatic breathing : Decreases breathing efficiency • pursed lip breathing Increases gaz exchange, increases tidal volume, reduces inspiratory time, reduces dyspnea, reduces end expiratory volumes Effectineness assessed by SaO2 Bianchi R, Gigliotti F, Romagnoli I. Chest wall kinematics and breathlessness during pursed-lip breathing in patients with COPD. Chest 2004 ; 125 : 459465. Breslin EH. The pattern of respiratory muscle recruitment during pursed-lip breathing. Chest 1992 ; 101 : 75-78
PULMONARY REABILITATIONExercise Training Specific strategries to increase training intensity O2 supplementation Controversial O2 supplementation - Reduces the ventilatory requirement for a given work rate • increases maximal exercises tolerance • Reduces exercise – ruduced pulmonary hypertension • Studies did not show additional benefit O2 could enhance training intensity in patients with COPD Funther studies
PULMONARY REABILITATIONExercise Training Specific strategies to increase training intensity Non invasive Mechanical Ventilation(NIMV) • reduces the inspiratory muscles load. • Usefulness only in severily impaired patients Hawkins P, Johnson LC. Proportional assist ventilation as an aid to exercise training in severe chronic obstructive pulmonary disease. Thorax 2002;57:853-859 Costes F, Agresti A, Noninvasive ventilation during exercise training improves exercise tolerance in patients with chronic obstructive pulmonary disease. J cardiopulm Rehabil 2003;23:307-313 • NIMV at home associated to out patient exercise training additional increase in the shuttle walk distance • QOL compared to training alone Garrod R, Mikelsons C Paul EA. Randomized controlled trial of domiciliary noninvasive positive pressure ventilation and physical training in severe chronic obstructive pulmonary disease. Am J Respir Crit Care Med 2000; 162:1335-1341
PULMONARY REABILITATIONExercise Training Specific strategies to increase training intensity Ergogenic drugs Anabolic steroïds (AS) • Studies included only men • Drugs studied areoxandrolone, nandrolone, stanozolol and testosterone • All studies report an increase in body weight through a gain in lean body mass 4 studies : AS + PRH program Muscle strength • Effects of strength training • does not improve exercise endurance (muscle hypertrophy without capillary and aerobic enzymes increase) • Protection against side effects of corticosteroïds NI prostate hypertrophy, aProstate cancer, Hb > 16g. Dl-1, Renal disease, Congestive heart failure Growth hormone/Insulin like growth hormone • Disturbed anabolic/catabolic balance in COPD • Lack of evidence of benefits – high cost • Schols AM, Soeters PB, Mostert R, Pluymers RJ. Physiologic effects of nutritional support and anabolic steroids in patients with chronic obstructive pulmonary disease : a placebo controlled randomized trial. Am J Respir Crit Care Med 1995;152 : 1268-1274
PULMONARY REABILITATIONComponents of the rehabilitation program • Smoking cessationthe key to the prevention and treatment of COPD • Give up • early stages interventions Reduced rate of FEV1 decline - Function lost is however not regained • Advanced disease, still valuable • Maintenance of abstinence : beyond the phase of acute withdrawal for extended periods thereafter
PULMONARY REABILITATION Smoking cessation Addiction - Nicotine substitutes - Psychological - Behavioral - Physiological Hard to accomodate the needs of every smoker Strategies Individual adapted programs Rather than group programs Pharmacological interventions Behavioral interventions
PULMONARY REABILITATION Education and self-management : Optimally control the disease Achive behavioral change Improve coping with the disease Up to 75 % of patients have difficulties in understanding how and when to take their inhalation medication Goodman DE, Israel E, Rosenberg M, Johnston R, Weiss ST, Drazen JM. The influence of age, diagnosis, and gender on proper use metered-dose inhalers. Am J Respir Crit Care Med 1994;150:1256-1261 Educational sessions - Improve adherence to medication - Help patients to deal with exacerbations - Reduce hospital days - Cost effective - QOL Helpful for patients with severe disease, Small groups-or individual Gallefoss F, Bakke PS. Cost-benefit and cost-effectiveness analysis of self-management in patients with COPD : a 1-year follow-up randomized, controlled trial. Respir Med 2002;96:424-431
PULMONARY REABILITATIONPsychosocial support Rationale : - Depression in COPD 2.5 fold higher/ general population - 20-40 % of COPD present with anxiety and depression - Spouses of COPD suffer from depression and stress - Smoking cessation result in mood disturbance. Psychological interventions improve mood distrubances > exercise training only. Can be associated to smoking cessation counselling, support and to education. Enhance the chances for sustained smoking cessation
PULMONARY REABILITATIONImproving activities of daily living Occupational therapy Occupational therapists interventions aim to increase the patient functional autonomy Methods consist of exercise training oriented toward daily living activities (walking efficiency, ventilatory capacity..) Wheeled devices (rollators) are useful but expensive They could be useful in severe diseases
PULMONARY REABILITATIONNutritional Programs - In COPD, - of body weight - Loss of fat-free mass is related to morbidity and mortality - > 2 kg of body weight improve survival - resting energy expenditure Exercise traing may induce a negative protein balance But– it is no sure that patients receiving nutritional supplements would not distrub their regular nutritional habits with a consecutive reduced calorie intake and risk of paradoxal undernourishment. - At the opposite, obese patients should undergo weight loss through a dietary intervention without loosing fat-free mass.
PULMONARY REABILITATION Miscellaneous - Erythropoietin therapy - antioxidant therapy (Vit E, Nacetyl cysteine) - Brondilators associated to PRH improvements in QOL - In selected subpopulations individualized programs - Does not concern all patients - Physiotherapy - sputum drainage
PULMONARY REABILITATIONUse of health care resources • Benefit of PRH is due to improved knowledge of the disease and enhanced self-management rather to physiological improvements • Admissions are reduced by 40 % when a self management program is followed despite significant physiological effects • No decrease in hospital days for long term exercise training without individualized education sessions and self management strategies. Engström CP. Long-term effects of a pulmonary rehabilitation programme in outpatients with chronic obstructive pulmonary disease : a randomized controlled study. Scand J Rehabil Med 1999;31:207-213. • Reduction in mild exacerbations may lead to stop disease progression • Exacerbation frequency linked FEV1 decline Donaldson GC. Relationship between exacerbation frequency and lung function decline in chronic obstructive pulmonary disease. Thorax 2002;57:847-852
PULMONARY REABILITATIONUse of health care resources ( cost-effectineness) • necessity of long – term following Reduction of hospitalization • Griffithsetal patients with COPD spent fewer days hospitalized during a 1 year follow-up period. Griffiths TL, Burr ML, Campbell IA. Results at 1 year of outpatient multidisciplinary pulmonary rehabilitation : a randomised controlled trial. Lancet2000 ; 355 : 362 - 368 • Out patients PRH reduces hospital days but studies lacked statistical power • Hospital days are the primary cost driver of COPD care Croxton TL, Weinmann GG, Senior RM. Clinical research in chronic obstructive pulmonary disease : needs and opportunities. Am J Respir Crit Care Med 2003 ; 167 : 1142 - 1149
PULMONARY REABILITATION Maintenance strategies Several strategies have been tried to maintain the benefits as long as possible after graduation from PRH programs - Continued 3 times weekly out patient 15 months - Once week high – intensity exercise training sessions - Exercise advise during the follow-up - Repeated short programs - Telephone support - Once monthly follow-up visits Maintenance programs seem to be necessary after 6 weeks out patients or 6 weeks in patients. After longer programs (6 months), benefits could be prolonged for > 1 year.
PULMONARY REABILITATION Survival No study has convincingly shown evidence of improved survival after PRH In 7 studies Best estimate :Rehabilitation reduces short-term risk of dying by 31 %. Not statistically significant ( nb of patients insufficient, patients on PRH are in a stable state) Further studies
Conclusion • In COPD muscle deficiency and flow limitation lead to deficiency and handicap • PR enhances exercise capacity, improves daily life activities and ameliorate QOL • A successful PR is scientific, transdisciplinary, individualised and sustained for at least 8 weeks • PR is cost effective • Further studies are needed for specific added stategies