Download
1 / 75
770 likes | 951 Views
PULMONARY. EMBOLISM. ALOK SINHA Department of Medicine Manipal College of Medical Sciences Pokhara , Nepal. Clinically significant obstruction of part or all of the pulmonary vascular tree, usually caused by thrombus from a distant site. Massive P E. Medium size P E. Small P E.

E N D
PULMONARY EMBOLISM ALOK SINHA Department of Medicine Manipal College of Medical Sciences Pokhara, Nepal
Clinically significant obstruction of part or all of the pulmonary vascular tree, usually caused by thrombus from a distant site
Massive P E Medium size P E Small P E
Incidence • Account for up to 15% of all post-operative deaths • Commonest cause of death following elective surgery • Commonest cause of maternal death • Improved diagnostic methods mean that it is probably reported more frequently
Pathophysiology 75% thrombi generated in deep venous system of the lower limbsand pelvis
Anti coagulant factor deficiencies • Auto immune disorders • Certain cancers • Platelet disorders • Smoking • Contraceptive pills • Heart failure • Increased viscosity • Small blood clots • Prolonged immobilization
Previously undiagnosed cancer is frequent in patients with unprovoked VTE prevalence of previously undiagnosed cancer in patients with unprovoked (idiopathic) VTE (venous thromboembolism) was 6.1% (95% CI, 5.0% to 7.1%) at baseline and 10.0% (CI, 8.6% to 11.3%) from baseline to 12 months risk of cancer was 4-fold greater in patients with unprovoked VTE (10%) than in those with a clear precipitating factor (2.6%) an extensive screening strategy using computed tomography of the abdomen and pelvis statistically significantly increased the proportion of previously undiagnosed cancer detected from 49.4% (CI, 40.2% to 58.5%) (with limited screening alone - history and examination, routine blood tests, CXR) to 69.7% (CI, 61.1% to 77.8%) in patients with unprovoked VTE Cancer and venous thromboembolism (VTE)
Inherited Thrombophilia (propensity to develop thrombosis due to an abnormality in the coagulation system ) • 25 - 50% of patients with VTE have an identifiable inherited thrombophilia • Antiphospholipid syndrome • Among the identified acquired thrombophilic states, it is the most common • lupus anticoagulant (LA) • anticardiolipin antibodies (ACA) • Deficiency of Protein C & S & antithrombin III small protein molecule that inactivates several enzymes of coagulation system • Factor V leiden COAGULATION COAGULATION - - - - Protein C & S Anti thrombin III Protein C & S Anti thrombin III + Factor V
These usually need to interact with an additional acquired risk factor to cause VTE Inherited thrombophilia Dehydration Pulmonary embolism (DVT) + =
Symptoms of DVT • Warmth, swelling, redness, and /or pain in a leg • DVT of the calf – symptoms in the calf • In thigh – symptoms in both thigh &/or calf • Vast majority of DVTs occurs in only one leg at a time • Other medical conditions can cause pain and/ or swelling in the legs
Thrombi can develop in • The heart following • Atrial fibrillation • Myocardial infarction • Prosthetic valve • Endocarditis • In association with intraventricular septal defects (paradoxical emboli) • AV shunts • With central venous access
Clinical features are: • Very varied • Non specific • Strong degree of suspicion required for diagnosis • All information has to be examined carefully before giving a verdict Wow ! What a geeeeniusyar !! I am “Saarlak Homes” Like a detective
The clinical features of PE depend upon • Size of embolism • Pre existing state of myocardium & lung parenchyma • Co-morbidity • Encompass a spectrum from Small emboli with few or no haemodynamic consequences Cardiovascular collapse
Thrombi/embolus can be Massive Medium Small
Large clot lodge at the bifurcation of the main pulmonary arteries causing haemodynamic compromise
Pathophysiology: • Major haemodynamic effects: • ↓ Cardiac output • Acute right heart failure Symptoms: • Severe dyspnoea • Faintness or collapse • Central chest pain • Apprehension on sitting up ? Platypnoea
(some times) • Isolated dyspnoea:Acute breathlessness in the absence of circulatory collapse • Suspect PE: sudden onset of unexplained breathlessness, in the presence of risk factors for VTE
Chest X-ray: • Usually normal. May be subtle oligaemia • Wester mark sign
ECG: • S1 Q3 T3 anterior T-wave inversion • Right bundle branch block (RBBB)
Right heart strain or acute cor pulmonale • Tall peaked p-waves in II,III,AVF • Right axis deviaton (S>R in lead I) • Right bundle branch block
Arterial blood gases: • Markedly abnormal with ↓ PaO2 and ↓ PaCO2 • Metabolic acidosis
Smaller clot travel more distally • May infarct lung • Pulmonary infarction is an uncommon consequence because of the bronchial arterial collateral circulation • Causes pleural involvement ± effusion Symptoms: • Pleuritic chest pain • Restricted breathing • Haemoptysis • Found most often in the lower lobes, where blood flow is greater
Some times • Collapse (clinical deterioration)(10%) • In an elderly patient with limited cardio respiratory reserve • Can rapidly decompensate with even a relatively small PE • Clinical findings non-specific and reflect the underlying disease process, rather than the PE itself
Signs: • Tachycardia • Pleural rub • Crackles or crepitations • Effusion (often blood-stained) • Low-grade fever
ECG: • Sinus tachycardia Arterial blood gases: • May be normal or ↓ PaCO2
Chest X-ray: • Pleuropulmonary opacities • Pleural effusion • Linear shadows • Raised hemidiaphragm
. X Ray findings
Pulmonary infarction – triangular opacity with base towards periphery – Hamptons sign
Chronic PE Pathophysiology: • Chronic occlusion of pulmonary microvasculature • right heart failure Symptoms: • Exertional dyspnoea • Late symptoms of pulmonary hypertension or right heart failure Signs: • May be minimal early in disease • Later-RV heave • loud, split P2 • Terminal-right heart failure
Chest X-ray: features of pulmonary hypertension • Enlarged pulmonary artery trunk • enlarged heart • prominent RV ECG: • RV hypertrophy and strain Arterial blood gases: • Exertional ↓ PaO2 or desaturation on formal exercise testing
DIAGNOSIS • DIFFICULT • Varied clinical features • Physical - signs non-specific • Lack of sensitive and specific diagnostic tests • Ask three questions: • Is the clinical presentation consistent with PE? • Does the patient have risk factors for PE? • Is there any alternative diagnosis that can explain the patient's presentation?
BTS PRE-TEST CLINICAL PROBABILITY SCORING • A. Patient has clinical features compatible with PE: • raised respiratory rate • ± haemoptysis • ± pleuritic chest pain • Plus 2 other factors: • 1. Absence of another reasonable clinical explanation • 2. Presence of a major risk factor • A. + 1 and 2 HIGH • A. + 1 or 2: INTERMEDIATE • A. alone: LOW pre-test clinical probability
In > 80% cases the X ray & ECG are normal • All patients with suspected PE should have • chest X-ray • ECG • arterial blood gas analysis • Help to exclude important differential diagnoses
Variety of radiographic appearances -usually non-specific • Suspect P E in • Normal X ray in an acutely breathless and hypoxaemic patient • bilateral changes in a patient presenting with unilateral pleuritic chest pain • Most important role of the chest X-ray is to exclude important D D • heart failure • pneumonia • pneumothorax • tumour
Arterial blood gases • Ventilation-perfusion mismatch and reduced cardiac output with a low mixed venous oxygen saturation and hyperventilation • Arterial blood gases show a • Reduced PaO2 and a normal or low PaCO2 • Normal in a significant minority • Metabolic acidosis may be seen in acute massive PE with cardiovascular collapse
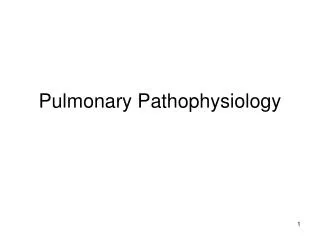
Bedside echocardiography extremely helpful in: • differential diagnosis • assessment of acute circulatory collapse • Acute dilatation of the right heart usually present in massive PE • Thrombus may be visible • Alternative diagnoses • left ventricular failure • aortic dissection • pericardial tamponade Can be established with confidence
Patient with acute pulmonary hypertension due to pulmonary embolism After clot lysis
SPECIFIC INVESTIGATIONS • D-dimer & other circulating markers • Ventilation-perfusion scanning • Pulmonary angiography • CTPA & MRPA
D-dimer • D-dimer: degradation product of fibrin undergoing endogenous fibrinolysis • Low D-dimer has a high negative predictive value useful screening test • Non-specific elevation of the D-dimer • myocardial infarction • pneumonia • sepsis • Suggestive clinical picture in a high-risk patient must be investigated further even when D-dimer level is normal