Download
1 / 31
330 likes | 816 Views
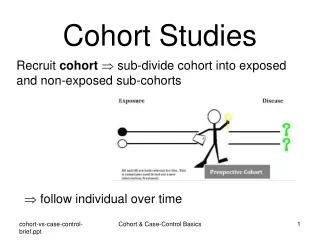
Cohort Studies for Outbreak Investigations. Goals. Describe the basic steps of conducting a cohort study. Discuss how to calculate measures of disease and disease association. Practice conducting basic analysis for an example outbreak.

E N D
Goals • Describe the basic steps of conducting a cohort study. • Discuss how to calculate measures of disease and disease association. • Practice conducting basic analysis for an example outbreak. • Provide examples of recent outbreak investigations that have used the cohort study design.
Quick Review of Cohort Studies • Useful when: • Defined population at risk for developing disease of interest • Possible to interview all members or representative sample of the cohort • Usually retrospective because exposure and enough cases to signal an outbreak have already occurred • Aim is to determine what exposures occurred in the past to cause cases of disease
Establishing the Cohort • Choose cohort members based on characteristics that assume exposure has occurred • Unexposed group must be similar to the exposed group in all respects except the exposure • Using groups that have other differences may lead to “confounding” • Cannot know whether difference in disease outcome due to exposure or the other differences
Establishing the Cohort • Or identify a population group and then determine whether they were exposed • People who happened to be at the same place at the same time • Attendance at an event • Membership in a particular group • Example: Athletes competing in the Eco-Challenge Sabah 2000 multi-sport race in Malaysia who developed illness after exposure to the Segama River. (1) • People who all belong to the same group or attend the same event are likely to be very similar to each other—confounding may not be a major issue
Conducting the Investigation • The exposure causing an outbreak is not always known • Investigators measure number of plausible exposures and evaluate each one • People who did/did not eat at a restaurant • People who did/did not use swimming facilities • People who did/did not get ice from ice machine • People who did/did not eat potato salad at picnic
Conducting the Investigation • Develop questionnaires and interview members of the cohort • Demographic information • Exposure to any potential risk factors for disease • Determine which cohort members meet the case definition • Analyze information to determine whether there is a relationship between exposure and disease
Analyzing Data—Prevalence • Prevalence = number of ill people divided by the total population at risk (the cohort) at a particular point in time • Often expressed as a percent • Example: in 1993, the prevalence of chronic fatigue syndrome among patients attending a primary care physician was 3%. (2)
Analyzing Data—Risk • Risk = probability of acquiring disease • Example: The risk of acquiring HIV from a blood transfusion in the U.S. is approximately 0.0002% (3) • Risk = number of cases divided by total population (cases and non-cases) • Can calculate risk in cohort because you know the number of people at risk of developing disease • Cannot calculate risk in a case-control study because includes only a sample of people at risk or may not know number of people at risk • Also called attack rate • Example: an influenza epidemic in a nursing home had an attack rate of 83% (43 of 52 residents became ill) (4)
Analyzing Data—Risk Ratio • Risk can be calculated separately for exposed and unexposed groups • Known as risk ratio (RR) or relative risk: the risk of one group relative to the risk of another group • Risk Ratio = the risk in exposed group divided by the risk in unexposed group
Analyzing Data—2x2 Table • Risk and Risk Ratios: 2x2 table
Analyzing Data—Risk Ratio • To interpret RR, compare the value to 1 • If risks in both groups are the same, RR will be 1, indicating no association between the exposure and the risk of disease • If RR = 1, no association with disease • If RR > 1, exposure positively related to disease • If RR < 1, exposure inversely related to disease • Example: In an outbreak of histoplasmosis in a high school, the risk ratio for students in classrooms near the courtyard during rototilling was 1.3, meaning that the risk of illness for students near the courtyard was 1.3 times the risk of illness for students not near the courtyard. (5)
Practice Calculating Risk • 61 children who attended Daycare X taken to the zoo, given boxed lunches • Over next few days, several children became ill and 6 culture-confirmed with Salmonella Enteritidis • Case defined as any child or adult attending the Zoo Day trip of Daycare X presenting with diarrhea, abdominal cramps, and/or fever within 72 hours of the trip. • 27 children met case definition
Practice Calculating Risk • The overall risk of illness among children: # ill = 27 = 0.44 = 44% total # children 61
Practice Calculating Risk • All children and adults asked which animal exhibits they visited, whether they participated in the petting zoo, what lunch and snack items they ate
Practice Calculating Risk • Selected exposures from children attending Daycare X Zoo Day
Practice Calculating Risk • Many sick children ate turkey sandwich, so let’s focus on that exposure: • 35 of the 61 children reported eating at least part of turkey sandwich = EXPOSED group • 26 children reported NOT eating any of the turkey sandwich = UNEXPOSED group • 21 of 35 exposed children became ill • 6 of the 26 unexposed children became ill
Practice Calculating Risk • 2x2 table showing exposure to the turkey sandwich by illness status
Practice Calculating Risk • Calculate risk of illness among those exposed to turkey: # ill exposed = 21 = 0.60 = 60% total # exposed 35 • Calculate risk of illness among those NOT exposed to turkey: # ill unexposed = 6 = 0.23 = 23% total # unexposed 26
Practice Calculating Risk • Risk of illness among exposed = 60% • Risk of illness among unexposed = 23% • Calculate risk ratio: risk among the exposed = 0.60 = 2.61 risk among the unexposed 0.23
Practice Calculating Risk • RR of 2.61 shows that the risk of acquiring Salmonella among those who ate turkey was 2.61 times the risk of acquiring Salmonella among those who did not eat turkey • Strength of association will be discussed in future issue of FOCUS
Practice Calculating Risk • If the turkey sandwich was responsible, why were there cases among the not exposed? • People (especially children) may have forgotten that they ate the turkey sandwich • Cross-contamination may have occurred during food preparation or while the children were eating • Secondary transmission could have occurred between children at the daycare • Unexposed children could have become ill by chance regardless of Zoo Day
Practice Calculating Risk • So have you found the culprit? • Even after we find an association between an exposure and disease, we should examine other potential exposures for other significant associations • Next, we should attempt to find the source of contamination (A future issue of FOCUS will describe how to conduct a traceback investigation)
Example Cohort Study: Gastroenteritis at a tourist resort • July 2000: outbreak of gastroenteritis at tourist resort in southern Italy (6) • Illness identified in 344 people, including 69 staff members • Retrospective cohort study performed to assess risk factors associated with illness in staff members
Example Cohort Study: Gastroenteritis at a tourist resort • July 2000: outbreak of gastroenteritis at a tourist resort in southern Italy (6) • Illness identified in 344 people, inlcuding 69 staff members • Retrospective cohort study among staff • Attack rate among staff = 38.1% (69 of 181); highest in waiters, sports trainers, entertainers, cleaning staff • Relative risks significant for exposure to beach showers (RR=1.8) and consuming drinks with ice (RR=1.8)
Example Cohort Study: Foodborne outbreak at a restaurant • December 2000-January 2001: health authorities in southwest Germany contacted by ill persons about gastroenteritis symptoms (7) • Part of four independent parties who attended luncheons at a particular restaurant • All 40 attendees at the four luncheons asked to participate in a cohort study • Of 30 persons who returned questionnaires, 26 met clinical case definition; attack rate = 87% • Only food item with statistically significant association with disease was a side salad (RR=5)
Example Cohort Study: Gastroenteritis on a cruise ship • July 2004: Alaska Department of Environmental Conservation notified the Alaska Section of Epidemiology of several cases of gastroenteritis among passengers on a cruise ship in Prince William Sound; additional report of laboratory-confirmed case of Vibrio parahaemolyticus that started while on the same ship (8) • Retrospective cohort study on passengers from four July 2004 cruises on the same ship • 189 passengers in cohort, 132 interviewed, 22 met case definition (attack rate = 17%) • Attack rate for persons who ate oysters = 29% (14 of 48)
Example Cohort Study: MRSA outbreak on football team • September 2003: Connecticut Department of Public Health notified about cluster of Methicillin-resistant Staphylococcus aureus among members of a college football team (9) • Retrospective cohort study of the 2003 team • 90 of 100 players interviewed; 10 met case definition (attack rate = 10%) • Highest risk among cornerback defensive backs (RR = 17.5), wide receivers (RR = 11.7), players with turf burns (RR = 7.2), players who reported body shaving (RR = 6.1)
References 1. Centers for Disease Control and Prevention. Update: outbreak of acute febrile illness among athletes participating in Eco-Challenge Sabah 2000 — Borneo, Malaysia, 2000. MMWR Morb Mortal Wkly Rep. 2001;50:21-24. 2. Bates D, Schmitt W, Buchwald D, et al. Prevalence of fatigue and chronic fatigue syndrome in a primary care practice. Arch Intern Med. 1993;153:2759-2765. 3. Centers for Disease Control and Prevention. How safe is the blood supply in the United States? Available at: http://www.cdc.gov/hiv/pubs/faq/faq15.htm. Accessed December 5, 2005.
References 4. Infuso A, Baron S, Fauveau H, et al. Value of influenza vaccine during an outbreak of influenza A in a nursing home, Pyrénées Atlantiques, France, November-December 1995. Euro Surveill. 1996;1(5):35-37. 5. Chamany S, Mirza SA, Fleming JW, et al. A large histoplasmosis outbreak among high school students in Indiana, 2001. Pediatr Inf Dis J. 2004; 23:909-914. 6. Boccia D, Tozzi AE, Cotter B, et al. Waterborne outbreak of Norwalk-like virus gastroenteritis at a tourist resort, Italy. Emerg Infec Dis. 2002;8:563-568.
References 7. Doller PC, Dietrich K, Filipp N, et al. Cyclosporiasis outbreak in Germany associated with the consumption of salad. Emerg Infec Dis. 2002;8:992-994. 8. McLaughlin JB, DePaola A, Bopp CA, et al. Outbreak of Vibrio parahaemolyticus gastroenteritis associated with Alaskan oysters. N Engl J Med. 2005;353:1463-1470. 9. Begier EM, Frenette K, Barrett NL, et al. A high-morbidity outbreak of methicillin-resistant Staphylococcus aureus among players on a college football team, facilitated by cosmetic body shaving and turf burns. Clin Infect Dis. 2004;39:1446-1453.