Download
1 / 41
420 likes | 582 Views
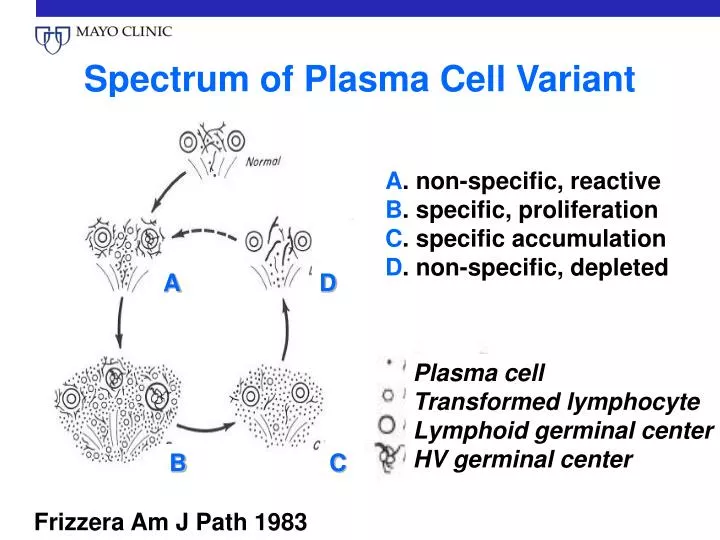
Plasma cell Transformed lymphocyte Lymphoid germinal center HV germinal center. Spectrum of Plasma Cell Variant. A . non-specific, reactive B . specific, proliferation C . specific accumulation D . non-specific, depleted. A. D. B. C. Frizzera Am J Path 1983.

E N D
Plasma cell Transformed lymphocyte Lymphoid germinal center HV germinal center Spectrum of Plasma Cell Variant A. non-specific, reactive B. specific, proliferation C. specific accumulation D. non-specific, depleted A D B C Frizzera Am J Path 1983
Histologic Differential Diagnosis • Thymomas • Angioimmunoblastic lymphadenopathy • Other atypical lymphoproliferations • Primary or acquired immunodeficiencies • Autoimmune diseases • In association with malignancies
CD: Outline • History • Histology • Pathogenesis • Clinical aspects • Treatment • Future directions
Histology Therapy Castleman Disease Uni- v. Multi-centric KSV HIV Other Cytokines
Interleukin 6 • Removal of CD LN mass IL-6drop and resolution of symptoms • Yoshizaki K et al. Blood 1989;74:1360-7. • Overexpression of IL-6 in mice produces a phenotype similar to MCD • Brandt SJ, et al. Curr Top Microbiol Immunol 1990;166:37-41. • Treatment with IL-6 receptor antibody relieves symptoms and signs • Nishimoto N et al. Blood 2005;106:2627-32.
Cells of Interest • Stroma: follicular dendritic reticulum cells • Dysplasia • IL-6 • Lymphoplasmacytic compartment: • Clonal? • Lymphocytes: no • Interfollicular plasma cells: maybe • Plasmablasts, monotypic: maybe
Human Herpes Virus 8 (HHV-8) a.k.a. Kaposi’s Sarcoma Virus (KSV) • Present in nearly 100% of HIV associated MCD • Present in 20-40% of HIV negative MCD patients • Both latent & lytic protein expression • vIL-6 produced in lymphoid cells
CD: Outline • History • Histology • Pathogenesis • Clinical aspects • Treatment • Future directions
Castleman DiseaseBackground • Spectrum of symptoms and disease course is variable… • Ranging from • Asymptomatic to… • Compressive adenopathy to… • A complex life-threatening syndrome with autoimmune/ inflammatory features
HV PC Multicentric Unicentric 10% 8% HV PC Unicentric Multicentric 39% 38% Mixed Mixed Multicentric Unicentric 2% 3% Relationship of ‘Centricity’ and Histology, n = 114 Dispenzieri et al, submitted
Mixed-Uni/ multi n=5 1.0 0.8 0.6 PC-Unicentricn=11 0.4 Surviving 0.2 0.0 0 3 6 9 12 15 18 21 24 27 30 Years follow up Effect of ‘Centricity’ and Histology on Survival, n = 114 HV-Unicentric n=45 HV-Multicentricn=9 PC-Multicentric n=44 P=0.06 Dispenzieri et al, submitted
Baseline Characteristics 114 CD Patients Mayo & U. Neb Dispenzieri et al, submitted
Baseline Characteristics114 CD Patients Mayo & U. Neb Dispenzieri et al, submitted
Baseline Characteristics114 CD Patients Mayo & U. Neb Dispenzieri et al, submitted
OS: Univariate Predictors, n=114 Dispenzieri et al, submitted
Platelets N MS, yr Normal 57 NR Low 10 6.2 Elevated 27 5.6 Respiratory Sx. N MS, yr None 92 NR Present 22 5.2 Organomegaly N MS, yr None 95 NR Present 19 6.2 1.0 0.8 1.0 Surviving 1.0 0.6 Surviving 0.8 Surviving 0.4 0.8 P = 0.0001 HR = 1.8 (1.2-2.6) 0.6 0.2 P = 0.01 HR = 1.6 (1.1-2.2) P = 0.003 HR = 1.8 (1.2-2.6) 0.4 0.6 0.0 Years follow up 0 3 6 9 12 15 18 21 24 27 30 0.2 Years follow up Years follow up 0.4 0.0 0.2 0 3 6 9 12 15 18 21 24 27 30 0 3 6 9 12 15 18 21 24 27 30 0.0 Dispenzieri et al, submitted
100 No Peripheral neuropathy (n=31) Peripheral neuropathy (n=25) 80 60 ‡ 40 20 ‡ ‡ * * 0 † ‡ † † Anemia Skin abn. Extravascular overload Papilledema Polycythemia Sclerotic bone Organomegaly Endocrine abn. Thrombocytosis Plasma cell variant Thrombocytopenia Respiratory sx/sign MCD-Symptoms/Signs Based on Absence or Presence of PN % of patients with or without PN with given attribute *P<0.0001; †, <0.01; ‡, <0.05 Dispenzieri et al, submitted
1.0 0.8 0.6 0.4 PN patients N MS, yrs With bone lesion 11 NR Without bone 19 5.4 0.2 0.0 0 3 6 9 12 15 18 21 24 27 30 Surviving HR 2.7 (1.5-5.7) P=0.0006 Follow-up in years Dispenzieri et al, submitted
O S M CD+ PN CD + POEMS OSM + POEMS CD+ POEMS +OSM CD Overlap Among CD, POEMS, & Osteosclerotic Myeloma CD, Castleman’s Disease PN, peripheral neuropathy OSM, osteosclerotic myeloma POEMS, peripheral neuropathy, organomegaly, monoclonal protein, skin D
1.0 Surviving 0.8 0.6 0.4 Follow up in years 0.2 0.0 0 3 6 9 12 15 18 21 24 27 30 Score N MS, yr 1 40 NR 2 35 11.5 3-4 19 3.6 1 POINT EACH FOR: Abnormal platelets No sclerotic bone Respiratory sx Peripheral neuropathy HR 3.6 (2.2-6.0) P<0.0001 Age adjusted HR 4.1 (2.4-7.5)
Predictors of Disease Variability Histology Therapy Castleman Disease Uni- v. Multi-centric KSV HIV Other Cytokines
Castleman Disease Associated Diseases • Paraneoplastic pemphigus • Bechet’s disease • Bronchiolitis obliterans • AA amyloidosis • Renal disease • POEMS syndrome • Autoimmune cytopenias • Lymphoma
CD and Lymphoma and Other Secondary Malignancies • HIV+ population • NHL 15-fold of HIV+ population w/o CD • HIV-negative population • 1/3 develop malignancies, most notably lymphoma and Kaposi sarcoma • Both unicentric and multicentric patients appear to be a risk
CD: Outline • History • Histology • Pathogenesis • Clinical aspects • Treatment • Future directions
80 70 60 50 40 30 Unicentric, n=50 20 10 Multicentric, n=54 0 Percent Other Surgery Radiation Observation Prednisone Chemotherapy Choice of Therapies 104 CD Patients Mayo & U. Neb Dispenzieri et al, submitted
Irradiation for Castleman’s Disease • 21 UCD in literature, >70% responded • 6 MCD in literature all responded
Resect Irradiate Unicentric versus multicentric? Unicentric Multicentric Resectable? Systemic therapy required Yes No HIV positive? Yes No Vinblastine Liposomal doxorubicin Oral etoposide Rituximab Thalidomide Interferon Alkylator ± prednisone Alkylator ± prednisone Combination chemotherapy Rituximab Interferon Thalidomide Anti- IL-6 or -IL-6 receptor PBSCT Dispenzieri A, In press.
CD: Outline • History • Histology • Pathogenesis • Clinical aspects • Treatment • Future directions
HV v. PC HIV Uni- Multi- Castleman Disease Rx Cyto- kines KSV Other Future Directions/Conclusions • Median overall survival is 13 years • Simple surrogates—platelet, respiratory sx, organomegaly, peripheral neuropathy, sclerotic bone lesions—predict for outcome • Histopathology is less important than other factors • These prognostic features may provide insight in pathogenesis and outcome
Future Directions • Using updated technologies, molecular classification • Understand cytokine networks driving disorder • Formally study therapeutic approaches
HIV and CD • HIV + CD patients are more likely to have: • Multicentric disease • Mixed HV / PC variant • Peripheral lymphadenopathy • Systemic symptoms • Leukopenia and thrombocytopenia • Pulmonary symptoms • HHV-8 co-infectivity & clinical KS • 15-fold risk of developing NHL Oksenhendler. AIDS 1996;10(1):61-7. Oksenhendler. Blood 2002;99(7):2331-6. Loi S. HIV Medicine 2004;5(3):157-62.
Respiratory Sx. N MS, yr None 92 NR Present 22 5.2 Organomegaly N MS, yr None 95 NR Present 19 6.2 1.0 0.8 1.0 0.6 Surviving 0.8 Surviving 1.0 1.0 0.4 0.6 0.8 0.8 0.2 P = 0.01 HR = 1.6 (1.1-2.2) P = 0.003 HR = 1.8 (1.2-2.6) 0.4 0.6 0.6 0.0 0 3 6 9 12 15 18 21 24 27 30 0.2 0.4 0.4 Years follow up Years follow up 0.2 0.0 0.2 Mixed, n=5 Unicentric, n=58 MS, NR Hyaline vascular, MS, NR n=54 0.0 0.0 0 0 0 3 3 3 6 6 6 9 9 9 12 12 12 15 15 15 18 18 18 21 21 21 24 24 24 27 27 27 30 30 30 Surviving Multicentric, n=56 MS, 7.8 yr Surviving Plasma cell, MS, 8.8 yr n=55 P=0.06 HR 1.4 (1.0-2.0) P=0.003 HR 1.7 (1.2-2.6) 500 Years follow-up Years follow-up A B C D Dispenzieri et al, submitted
1.0 Surviving 0.8 0.6 Years follow up 0.4 0.2 0 3 6 9 12 15 18 21 24 27 30 0.0 PN N MS, yr No 84 NR Yes 30 7.5 P=0.022 HR =1.46 (1.0-2.0) Dispenzieri et al, submitted
Months Months Risk of Lymphoma in HIV+ CD Patients Survival from NHL diagnosis in 14 patients with MCD-associated NHL NHL in HIV-associated MCD in 60 HIV-infected patients Oksenhendler Blood 99:2331-2236; 2002
*Sclerotic bone lesions patients (n=11) excluded since associated with a risk of death of 0.5 (95%CI 0.3-0.9) Dispenzieri et al, submitted
Score N MS, yr 0 3 NR 1 27 11.4 2-3 23 5.8 Surviving 1.0 0.8 HR 4.0 (1.6-7.5) P= 0.0008 Age adjusted HR 3.1 (1.5-6.9) 0.6 0.4 1.0 Follow up in Years Score N MS, yr 0 47 NR 1 11 6.7 0.2 0.8 0.0 0.6 Surviving 0 3 6 9 12 15 18 21 24 27 30 0.4 HR 8.3 (2.1-40.3) P= 0.003 Age adjusted HR 6.3 (1.6-30.4) 0.2 0.0 0 3 6 9 12 15 18 21 24 27 30 Follow up in years I J Dispenzieri et al, submitted