Download
1 / 30
370 likes | 765 Views
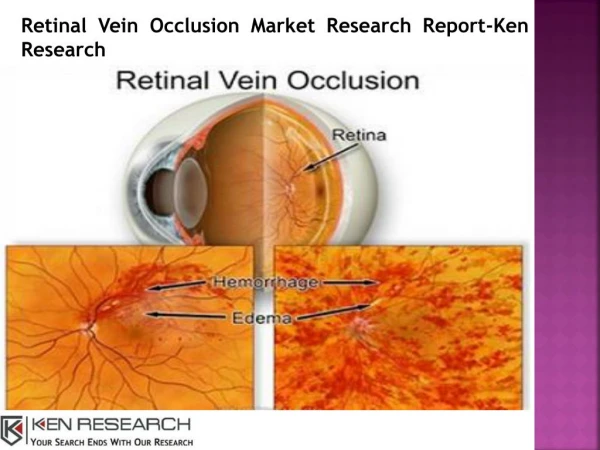
Retinal Vein Occlusions. Morphology. CRVO BRVO Hemispheric VO Hemicentral VO Papillophlebitis Macular BRVO. CENTRAL RETINAL VEIN OCCLUSION.

E N D
Morphology • CRVO • BRVO • Hemispheric VO • Hemicentral VO • Papillophlebitis • Macular BRVO
CENTRAL RETINAL VEIN OCCLUSION • The actual mechanisms producing the clinical picture of central retinal vein occlusion may be roughly divided into those conditions that produce a physical blockage at the level of the lamina cribrosa, and those conditions in which hemodynamic factors result in an obstruction to the flow of blood. These mechanisms probably coexist in many patients with central VO. "Blood and thunder" appearance of a central retinal vein occlusion.
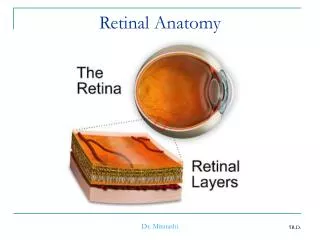
PATHOLOGY • Histopathologic evaluation of eyes removed because of a central retinal vein occlusion demonstrates an occlusion at or just behind the level of the lamina cribrosa. • At this location, there are certain anatomic factors that predispose the central retinal vein to occlusion. First, the lumina of the central retinal artery and central retinal vein are narrower than they are in the orbital optic nerve, and the vessels are bound by a common adventitial sheath.
Doppler Studies • Recently, color Doppler ultrasound imaging has been used to examine the blood flow in the orbit, including the optic nerve head, and has been used to examine patients with central retinal vein occlusion. • As might be expected, the venous velocity in the eye of a patient with central retinal vein occlusion is markedly reduced compared either with the unaffected eye or to control eyes. • There is evidence, however, that the central retinal artery blood flow is also impaired in eyes with acute central retinal vein occlusion. • In addition, vascular resistance is slightly higher in the ophthalmic artery and short posterior ciliary arteries of both the involved and the clinically healthy fellow eye of patients with central retinal vein occlusion compared with control eyes. • There is also a trend toward higher vascular resistance of the central retinal artery in the clinically healthy eyes of patients with central retinal vein occlusion compared with control eyes.
Risk Factors • An increased risk of central retinal vein occlusion was found in patients with systemic hypertension, diabetes mellitus, and open-angle glaucoma; the risk of central vein occlusion was decreased for patients with increasing levels of physical activity and increasing levels of alcohol consumption. • For women, the risk decreased with the use of postmenopausal estrogen and increased with a higher erythrocyte sedimentation rate. The Eye Disease Case-Control Study Group: Risk factors for central retinal vein occlusion. Arch Ophthalmol 114:545, 1996
Investigations • All patients with central retinal vein occlusion should have a comprehensive ophthalmic evaluation, including an appropriate evaluation for glaucoma. In addition, they should be referred to their primary care physician for an evaluation of cardiovascular risk factors, including hypertension and diabetes • GENERAL PRINCIPALS • Maximise Recovery and Vision • Prevent re-occlusion • Detect associated systemic disease • Detect / Prevent Glaucoma • Protect other eye
Standard Investigations • FBC, PV, ESR • U+E, Creatinine • LFT, Protein Electrophoreseis • Random Glucose, Lipid • Urine analysis
Ophthalmic Investigations • FFA • CDI (Color doppler ) • Carotid disease-Using digital subtraction angiography, Brown and associates studied 37 patients with central retinal vein occlusion; they found that significant ipsilateral stenosis (greater than 50%) was not higher in these patients compared with historically matched controls. They did find, however, that patients with ischemic central retinal vein occlusion had a higher incidence of overall carotid atherosclerotic obstruction (ipsilateral and contralateral) than patients with nonischemic central retinal vein occlusion
Ischemic Central Retinal Vein Occlusion • Patients with an ischemic pattern are usually aware of a sudden, painless decrease in visual acuity. Vision ranges from 20/400 to hand movements. The onset, however, is generally not as rapid or the visual loss as extensive as in central retinal artery occlusion. Exceptional cases have been noted in which patients with an acute onset had reasonably good vision and yet demonstrated a picture of ischemic central retinal vein occlusion. Patients with ischemic occlusion have an average age of 68.5 years.
Nonischemic Central Retinal Vein Occlusion • Nonischemic central retinal vein occlusion is a much milder and more variable disease in appearance, symptoms, and course compared with ischemic central retinal vein occlusion. Patients with nonischemic central retinal vein occlusion are an average of 5 years younger (average age, 63 years) than those with ischemic vein occlusion
Angiography • The intravenous fluorescein angiogram pattern of an ischemic central retinal vein occlusion is usually characterized by a delayed filling time of the venous tree of the retina, capillary and venous dilation, and extensive leaking of fluorescein into the retina, particularly in the macular area and in the area adjacent to the larger venous trunks and capillary nonperfusion may not be noted at the time of initial occlusion, but are usually manifest shortly thereafter. Late-phase photographs show patchy extravascular areas of fluorescence and staining of the retinal veins. The intravenous fluorescein angiogram pattern of an ischemic central retinal vein occlusion is usually characterized by a delayed filling time of the venous tree of the retina, capillary and venous dilation, and extensive leaking of fluorescein into the retina, particularly in the macular area and in the area adjacent to the larger venous trunks and capillary nonperfusion • Microaneurysms may not be noted at the time of initial occlusion, but are usually manifest shortly thereafter. • Late-phase photographs show patchy extravascular areas of fluorescence and staining of the retinal veins. Fluorescence in the macula indicates capillary leakage and edema; this not only may account for much of the initial visual loss in the acute phase, but may eventually result in permanent structural changes.
Classifying ischaemia • The amount of nonperfusion or ischemia is determined by inspecting the fluorescein angiography negative under magnification. The photographer inspects not only the central 30° or 45°, but as much of the peripheral retina as possible. • Another method has been to classify eyes with less than 10 disc diameters of perfusion on fluorescein angiography as perfused or nonischemic, and eyes with 10 or more areas of nonperfusion as nonperfused or ischemic.
Macular Oedema • Fluorescence in the macula indicates capillary leakage and edema; this not only may account for much of the initial visual loss in the acute phase, but may eventually result in permanent structural changes.
Prognosis CRVO • The prognosis for ischemic central retinal vein occlusion is generally poor because of decreased visual acuity and neovascularization. Visual loss occurs because of macular edema, capillary nonperfusion, overlying hemorrhage (either retinal or vitreal), or a combination of all of these. Retinal edema usually gradually subsides except in the macula, where it may persist for many months or years. Macular holes or cysts may form.
Neovascularization • The most serious complication of central retinal vein occlusion is neovascularization. • Neovascularization elsewhere (NVE) occurs less frequently than neovascularization of the iris (NVI), and usually only in ischemic occlusions. • The low incidence of retinal surface neovascularization in ischemic central retinal vein occlusion is thought to be due to the destruction of endothelial cells, which provide the source for endothelial proliferation and neovascularization.
Neovascularization of the Iris. • Neovascularization of the iris and frequently neovascular glaucoma occurs in approximately 8%6to 25% of all central retinal vein occlusions and generally only in those eyes that exhibit an ischemic pattern of occlusion. • Magargal and co-workers have shown that the incidence of neovascularization increases dramatically above approximately 50% capillary nonperfusion. The incidence of anterior segment neovascularization in nonischemic central retinal vein occlusion is approximately 1%, compared with approximately 35% to 45% for ischemic central retinal vein occlusion. • Neovascularization of the iris or angle is significantly correlated with the extent of capillary nonperfusion on the fluorescein angiogram. • Rubeosis developed in 80% to 86% of the eyes with severe nonperfusion of three to four quadrants of the posterior pole or the periphery, but in only 3% to 9% of those with less capillary nonperfusion.
HEMICENTRAL AND HEMISPHERIC RETINAL VEIN OCCLUSION • The terms hemicentral retinal vein occlusion and hemispheric retinal vein occlusion refer to eyes in which approximately half of the venous outflow from the retina, either the superior or the inferior, has been occluded. In approximately 20% of eyes, the branch retinal veins draining the superior and inferior halves of the retina enter the lamina cribrosa separately before joining to form a single central retinal vein. • Hemicentral retinal vein occlusion is an occlusion of one of these dual trunks of the central retinal vein within the nerve. Hemispheric retinal vein occlusion is an occlusion involving the venous drainage from approximately half of the retina, either the superior or the inferior retina
Hemispheric retinal vein occlusions • In some eyes, the nasal retina is not drained by a separate vein, but by a branch of either the superior or the inferior temporal vein. It is the occlusion of one of these veins draining both the nasal retina and the superior or inferior retina near the optic disc that accounts for the majority of hemispheric retinal vein occlusions. • The treatment and classification are similar to that of branch retinal vein occlusion.
BRANCH RETINAL VEIN OCCLUSION PATHOLOGY Leber was probably the first investigator to note the connection between branch retinal vein occlusion and the arteriovenous intersection. Koyanagi found that the majority (77.7%) of his cases of temporal vein occlusion involved the superior retina. He attributed this to the preponderance of arteriovenous crossings in this region compared with other quadrants.Others later confirmed this anatomic observation, noting that branch retinal vein occlusion always occurs at an arteriovenous intersection.Both fluorescein angiography1and histopathologic examination confirm that most occlusions occur at an arteriovenous crossing and that the few that do not are in the vicinity of a retinal artery. Histologically, where the vein and artery cross, they share a common adventitial sheath, and the venous lumen may be diminished by as much as a third at this crossing.
Morphology • The clinical picture of branch retinal vein occlusion is retinal hemorrhages that are segmental in distribution. • The apex of the obstructed tributary vein almost always lies at an arteriovenous crossing. Usually some degree of pathologic arteriovenous nicking is present. • The occlusion is commonly located one or two disc diameters away from the optic disc. However, the occlusion may lie at a point near the disc edge or, less frequently, may involve one of the smaller, more peripheral tertiary or macular branches.
Risk Factors for Branch Retinal Vein Occlusion • Systemic hypertension • History of cardiovascular disease • Increased body mass index at 20 years of age cholesterol • History of glaucoma • High serum levels of a2-globulin
Management of BRVO • Branch vein obstruction is often associated with pre-existing vascular disease. Evaluation for systemic abnormalities, in particular hypertension, should be performed. Exclusion of diabetes, hyperlipidaemia, hyperviscosity/coagulation states, antiphospholipid syndrome, or any other predisposing condition should be performed. Regular review is required until the haemorrhages clear so that the most suitable treatment option can be achieved. Approximately one third to one half of patients with BRVO have recovery of visual acuity to 20/40, or better, without therapy.
An important complication of branch retinal vein occlusion is neovascularization • Neovascularization of the iris and neovascular glaucoma are uncommon and occur in only approximately 1% of affected eyes. • More commonly, neovascularization of the disc occurs in approximately 10% of eyes, and neovascularization elsewhere occurs in approximately 20% of eyes. Generally, retinal neovascularization occurs within the retinal area served by the occluded vessel, but it has been reported to occur outside in presumably normal retina. • Vitreous hemorrhage due to neovascularization occurs in approximately half of the eyes with neovascularization.Butner and McPherson239 found that 11.3% of spontaneous vitreous hemorrhages were due to a branch retinal vein occlusion, an incidence second only to proliferative diabetic retinopathy as a cause of vitreous hemorrhage. • Oyakawa and co-workers found that in 38.3% of eyes undergoing a vitrectomy for a nondiabetic vitreous hemorrhage, the hemorrhaging was due to a branch retinal vein occlusion.
MACULAR BRANCH RETINAL VEIN OCCLUSION • An occlusion limited to a small venous tributary draining a section of the macula and located between the superior and inferior temporal arcades is considered a subgroup of branch retinal vein occlusion.Most patients with macular branch vein occlusion complain of blurring or distortion of vision. Superior macular vein occlusions are more common than inferior macular vein occlusions, and some degree of macular edema is present in approximately 85% of these eyes. • Although small areas of capillary nonperfusion are present in approximately 20% of eyes, neovascularization is not seen. This type of macular vein occlusion can be remarkably subtle at times. Joffe and associates pointed out that clues such as small collateral channels and microaneurysms often suggest the diagnosis. Treatment of macular edema in macular vein occlusion by photocoagulation is identical to the treatment of other branch retinal vein occlusion.
Investigations and therapy • GENERAL PRINCIPALS • Maximise Recovery and Vision • Prevent re-occlusion • Detect any associated systemic disease • Detect / Prevent Glaucoma • Protect other eye