Download
1 / 11
110 likes | 397 Views
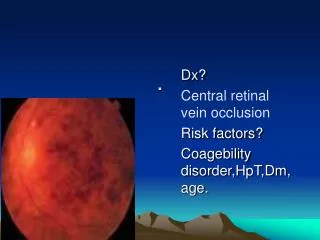
RETINAL VEIN OCCLUSION. Epidemiology. 51% >65y 10-15% <45y ν Afro-caribbean and Asian descent in UK. Pathogenesis Primary retinal venous disease/ endothelium Thrombus secondary event (Hypercoaguability). AETIOLOGICAL CONDITIONS. DIAGNOSIS. Painless loss of vision- unilateral

E N D
RETINAL VEIN OCCLUSION Epidemiology 51% >65y 10-15% <45y ν Afro-caribbean and Asian descent in UK • Pathogenesis • Primary retinal venous disease/ endothelium • Thrombus secondary event (Hypercoaguability)
DIAGNOSIS • Painless loss of vision- unilateral • Asymptomatic
BRVO Arteriovenous crossings Macular branch (DD from diabetic maculopathy)
MECHANISMS OF VISUAL LOSS Ischaemic (direct- indirect) Exudative (macular oedema) 30% non-isch. Convert to ischaemic type first 4/12 Eyes at High Risc for Ischaemic Complications 1.RAPD 2. VA 3. FFA >10DD, 5-10 DD 4.Cotton wool spots >10, 5-10 5. Deep dark haem. (infarct) 6. Elderly ( rubeosis)
DIFFERENTIAL DIAGNOSIS 1.Accelerated hypertension 2.DM 3.Slow-flow retinopathy 4.Peripapillary telangiectasia 5. AION 6.Lupus/ radiation retinopathy 7. CMV retinitis 8.Ocular ischaemic syndrome
MEDICAL INVESTIGATIONS ALL PATIENTS FBC, ESR, U&E, LFT, GLC, Lipid profile Protein electrophoresis ECG TFT MORE SPECIALISED CXR Cardiolipin, Lupus anticoagulant CRP, ACE, FTA-ABS RF, ANA, DNA, ANCA MRI: orbit, brain
MANAGEMENT OCULAR BRVO Argon laser for macular oedema if foveal vasculature intact (FFA), VA 6/12-6/60 3-6/12 after the initial event Sectoral PRP for proliferative complications or if areas of non-perfusion >5DD FU: 6/52, up to 2years after (collaterals)
CRVO Prevention of neovascularisation Grid: no benefit FFA and Laser: haemorrhages sufficiently resolved Monthly FU/ total of 2years >40DD: PRP 10-40DD: no <10 (non-ischaemic): no Non-ischaemic cases convert to ischaemic 13%: 6/12 18%: 18/12 CHECK RAPD ALWAYS IN FU
MEDICAL • Maximise visual outcome • cardiovascular morbidity/ mortality (risk factors) • Prevent recurrence to other eye (15% over 5 years) + Aspirin/ dipyridamole