Download
1 / 39
400 likes | 580 Views
Perseverance is the hard work you do after you get tired of doing the hard work you already did. ~ Newt Gingrich. Anna White AP Spinal CMATS. Back Pain Pathway implementation by BCU. YLD 2013 DoH England. Causes of LBP Lancet 2018. National Back Pain and Radicular Pathway.

E N D
Perseverance is the hard work you do after you get tired of doing the hard work you already did. ~Newt Gingrich
Anna White AP Spinal CMATS Back Pain Pathwayimplementation by BCU
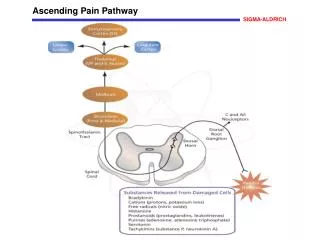
YLD 2013 DoH England Causes of LBP Lancet 2018
National Back Pain and Radicular Pathway • Prevent chronicity • Identify those at risk • Treat them quickly • Move them through the system quickly • Not treat the ones who don’t need it
Stakeholders • GP/ FCP- STarTBack & key messages • CMATS Spinal - TTP • Physiotherapy dept- quick & relevant treatments • Radiology- stop X-rays, quick MRI • Pain Clinic- Early intervention & root blocks • Tertiary centres- quick access
Challenges to Implementation & embedding • GP & FCP- STarTBack • Physio - waiting times/ STarTback/Treatment • CMAT- waiting times • Radiology waiting times • Pain Clinic and early intervention • Tertiary centres DATA: DATA:DATA
Functional Conditioning ProgrammeService Evaluation By Gemma Cartwright Clinical Specialist May 2019
Background • Persistent pain is defined as a complex and multifactorial phenomenon • Approximately 11-20% of adults report persistent pain that is moderately to severely disabling • Pain has a significant impact on individuals and their families and carers. Pain affects mood, sleep, mobility, role within the family, ability to work as well as other aspects of life. • The goal of persistent pain management has evolved looking at restoring the patient's physical and emotional function and overall quality of life How can we meet the needs of this population in the MSK physio setting? Functional Conditioning Team • Launched in January 2018 • Team of four clinicians working across four hospital sites and 3 community leisure centres to deliver the service
Functional Conditioning Programme • Four 2 hour sessions over a four week period • Based in the local leisure centres • Sessions consist of education and exercise • Education includes: - pain education - pacing - sleep - unhelpful thoughts - relaxation - stress - exercise/ effects of inactivity - Goal setting and barriers to change Alternative Treatment: • 1:1 sessions, hydrotherapy, one off pain education (1 hour)
Outcome measures • EQ5D- Looks at the patient’s health state looking at five dimensions: mobility, self-care, usual activities, pain/discomfort and anxiety/depression. • PSEQ- 10-item questionnaire, developed to assess the confidence people with ongoing pain have in performing activities while in pain • StartBack tool for stratifying care • Functional activity: 30 seconds STS Data was collected over a 6 month period
Results EQ5D • 42 full sets of data • 64.2% of patients self-scored that their overall health percentage had improved (average increase of 17.3%) PSEQ • 63.6% % of patients with completed data sets improved StartBack Tool • 71.4% of patients reported a lower STaRT back score when retested. Even though this isn’t a valid outcome score it could be suggestive that patients had less fear avoidance and catastrophyisation • 38% shift of patients who were deemed high risk at initial assessment
What have we taken from this? • Chronic Pain is multifactorial and therefore effective management involves a multidisciplinary approach considering all aspects of the patients health and lifestyle • PMP • Larger team
Redesigning a Rural Physiotherapy Service’s Documentation Audit Process: Improving Quality whilst Promoting Honest & Meaningful Conversations Andy Pellow MCSP Powys THB MSK Symposium 2019 MRC Llandrindod Wells
Background & Purpose • 2017 PTHB Physiotherapy Outpatients Notes Audit Review concluded “there is room for improvement” • The traditional audit process did not appear to be influencing the quality of the notes produced by the physiotherapy service • Evaluation of the traditional audit was too generic • Opportunity for the documentation audit process to have a bigger impact on practice/quality by highlighting good and bad practice in individuals, and by promoting honest conversations • This work explores the impact of the new audit process & tool
New Audit Tool & Process Excel tool Built in formulas produce an instant score with traffic light system Different audit tabs for each speciality Simple to use Comment section for justification of scoring (when needed) 1 set of notes audited during 90 day conversation/PADR (new staff audited once per month in first 3 months of employment) Each total score sent to project lead Service wide spreadsheet shows all audit scores for each physiotherapist
Staff Questionnaire Results 91% of responders feel that the new documentation audit tool is easy to use and they feel that the audit process has a direct impact on their record keeping Only 45% of the responders felt that the traditional, annual audit process had a direct impact. 73% of responders feel that doing the audit during 90 day reviews leads to wider discussion related to patient care and professional matters 36% of responders agree that the new audit process lead to discussions related to the wellbeing of the member of staff being audited, whereas 36% disagreed with this statement. 27% of responders remained neutral 91% of responders feel that the 90 day reviews are the best time to complete the documentation audit
Conclusions & Implications • New process has a greater impact on the clinical records that physiotherapists produce compared to the traditional, annual, documentation audit process • Staff value the one-to-one audit process and feel that this approach leads to wider discussion related to patient care and professional matters • Positive step forward in creating a supportive environment where staff feel they can have open and honest conversations • Potential for the new audit process to initiate and facilitate conversations related to the well-being of the Physiotherapist being audited
The OAK Concept National Physiotherapy MSK symposium – June 2019 Dr Rob Letchford PhD Learning for Health Team ABUHB T&O Knee sub speciality Sam Haworth-Booth Physio Manager Dr Sally Lewis National Lead VBH Claire Jordon Education Nurse Dr Rob Letchford Physio Martin Dando Physio Mr John Lloyd Consultant Surgeon
Self efficacy Self Care Options Point Bracing bend Lake Diagnosis Injection Weir Education Springs There when I need it Creek Exercise Island OAK Isle of Weight loss Peer support Valley Wear & Tear Falls Total Bliss FEAR Bend Total Disaster Nothing else Creak
Person CMATS Community Primary care Physiotherapy Core interventions Education Orthopaedics
Person Community Services Primary care Physiotherapy CMATS Decision Aid Options Grid Knee OA class GP / self referral Community facilities Group sessions NERS & AWM Orthopaedics Adult Education Shared Decision Making
ABUHB Knee OA Class Exercise and Education Built on ESCAPE Pain Collaboration with NERS Self-efficacy GRCS
Thank you to “team OAK” Options Advice Knowledge Knee-MAN Back-MAN
CMATS ‘ONE STOP SHOP’ SHOULDER CLINIC Sally Priest Advanced Physiotherapy Practitioner BCUHB East - Wrexham Maelor Hospital
WHY? • Clinicians frustration with the service / pathway. • Pathway for shoulder referrals – • GP refers to CMATS &/or direct to radiology for U/S scan (high number of inappropriate referrals from GP referrals identified) • CMATS assessment & refer to radiology for U/S scan if indicated – including U/S guided injections if required. • Review appointment in CMATS to discuss results & arrange appropriate onward management • This pathway demonstrates inefficiencies – 3 appointments & extended timeframe from initial referral to definitive management - frustrating for patient & clinician.
HOW? • Dr Makarious Asprou & myself – Msc module in musculoskeletal ultrasound imaging completed. • Close working relationship / support with Radiology services / Consultant Radiologist – supervised scanning, competency sign off, clinical governance, IT support. • Bid for funds for U/S scanner – caused a long delay. • Successful bid through charitable funds – Awyr Las £80,000. • CMATS admin team support. • Communication with GP’s. • Service started in April 2019.
SO FAR SO GOOD! • Change in radiology pathway for GP referrals for U/S scan shoulders. • 2 months of the service in place. • Reduced demand on radiology services – reduced number of inappropriate referrals – patients will be scanned in secondary care in a more timely manner. • Patients will only receive investigation when clinically indicated. • The investigation is an adjunct to clinical assessment. • Very high patient satisfaction recorded on patient experience questionnaire – ‘One stop shop – brilliant. I work & have had so many appointments which mean time off work. Such a relief to be able to explain my history to one person, scanned by the same person & discuss management with one person.’ ‘Fantastic service’. ‘A very good investment for ultrasound scanner’. • Reduced number of patient appointments • Improved patient pathway – more timely management, enhances patient understanding & expectations, ultrasound guided injections. • Access to clinics / parking.
WHAT NEXT? • Audit – data collection. • Plan to extend service to include other MSK conditions – would require additional support for this. • Succession planning – staff training. • Continued links / communication / competency support from radiology. • TO SUMMARISE: - This service is a great example where demand management & prudent healthcare improves / enhances the patients pathway & experience. • THANK YOU!
An Early Rehabilitation Pathway for Patients with Fractured Distal Radius treated with Open Reduction & Internal Fixation.A Pilot. Sarah Thomson, Advanced Physiotherapy Practitioner Morriston Hospital, Swansea Bay University Health Board. MSK Symposium June 2019.
Aims of the Pilot: To identify if an early active mobilisation programme following ORIF for fractured distal radius would be; a) Effective for the Patient b) Efficient for the Health Board
Methodology: The New Pathway • Bulky bandage instead of backslab, provision of advice leaflet, therapist review at 2 Weeks, x-ray at 12 weeks. Part A: Comparison to literature • Outcomes: ROM, Strength, VAS, Quick DASH, PWHRE, EQ-5D, X-ray, Satisfaction. Part B: Comparison new with old pathway • Outcomes : Referral to plaster room, Physio, Radiology & Follow up appointment
Results Part A (Effectiveness) Part B (Efficiency)
Summary: New pathway • Is an efficient pathway for patient care. • Is effective in patient outcomes. • Is cost efficient for the Health Board. Other Pathways & Guidelines Pathways Carpal Tunnel Syndrome Mallet Trigger Finger/Thumb Ganglion De Quervain’sDupuytren’s (TBC) Thumb Arthritis Physio Walk-in Clinic Guidelines Orthopaedic Hand Therapy Plastic Surgery Hand Therapy Hand Goniometry