Download
1 / 41
1.01k likes | 2.68k Views
Pain pathway. Y Tang. IASP definition. “Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage.”. Pain. The pain experience has two dimensions:

E N D
Pain pathway Y Tang
IASP definition • “Pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage.”
Pain • The pain experience has two dimensions: • 1. Sensory/discriminative - allowing us to locate tissue damage • 2. Affective/aversive - ‘unpleasant’ and ‘emotional’ in the IASP definition. Avoid stimuli that can damage tissue.
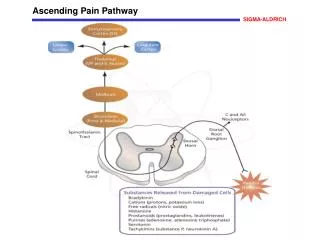
Ascending pain pathway • Those responsible for pain are called anterolateral system (also relays crude touch and temperature). • Dorsal column-medial lemniscal pathway mainly fine touch, vibration and position. • Somatosensory to cerebellum mainly for proprioception.
Anterolateral system • Contains at least 2 pathways: • Spinothalamic (a.k.a. direct/neospinothalamic) –pain/temp/crude touch. • Spinoreticular(a.k.a. indirect/paleospinothalamic) –’suffering pathway’/arousal in response to nociception. • Spinomesencephalic –pain modulation. • Spinotectal –initiating eye movement to painful stimuli. • Spinohypothalamic - autonomic and reflex responses to nociception.
Anterolateral system • Peripheral receptor – nerve ending of Aδ and C-fibres, detect stimulus. Signal carried by: • 1st order neuron – from periphery to spinal cord. Cell body in dorsal root ganglion, may travel up or down in ipsilateral spinal cord for several segments in the dorsolateral fasciculus (Lissauer tract), and then turn deeply to end in the dorsal horn. Then synapse with:
Anterolateral system • 2nd order neuron – cell body in dorsal horn. Decussates in anterior white commisure to the contralateral cord. Axons of spinothalamic tract ascend all the way to terminate in the thalamus. The other two tracts terminate at brainstem levels. Then synapse with: • 3rd order neuron – cell body in thalamus, ascend ipsilaterally to project to somatosensory cortex.
Peripheral receptor (Nociceptor) • Nerve endings of Aδ and C-fibres (80%) • Polymodal –mechanical, thermal, chemical. • Responds to high threshold stimuli.
First order neuron • Aδ primary afferents terminate in laminae I and V. • C primary afferents terminate in lamina II (substantia gelatinosa) and III. • Some 1st order neuron synapse with interneuron (95% dorsal horn neurones are interneurons-associated with reflex motor activity). • Axon of interneurons synapse with 2nd order neurons in laminae V-VIII
Second order neurons • Cell bodies in dorsal horn of spinal cord. • Direct –spinothalamic • Indirect –spinomesencephalic, spinotectal, spinohypothalamic.
2nd order neuron:Spinothalamic tract • Aδ fibres. • 15% nociceptive fibers from spinal cord terminate directly in thalamus via spinothalamic tract. • Consists of 2 anatomically distinct tracts; lateral (sharp pain and temp) and anterior spinothalamic tract (crude touch). Recent studies show all tracts in anterolateral system transmit nociceptive signals. • Projections to ventral posterior lateral nucleus of thalamus (also ventral posterior inferior and intralaminar nuclei). • Also has collaterals to reticular formation.
2nd order neuron: Spinoreticular tract • C fibres. • Some fibers decussate to contralateral side via anterior commisure, many ascend ipsilaterally. • Transmit nociceptive, thermal, crude touch signals from spinal cord to thalamus indirectly by forming multiple synapses in the reticular formation prior to their thalamic projections. • Some second order neurons bypass reticular formation and relay sensory input from C fibres directly to intralaminar nuclei of thalamus. • Reticular formation sends signals not only to thalamus but to hypothalamus (autonomic and reflex response), and the limbic system (mediate emotional component of nociception).
2nd order neuron: spinomesencephalic tract • Fibres terminate in periaqueductal grey matter and the midbrain raphe nuclei, both which give rise to fibres that modulate nociceptive transmission (‘descending pain-inhibiting system’). • Some other fibres terminate in parabrachial nucleus, which then sends fibres to amygdala (component of limbic system associated with processing of emotions).
2nd order neuron: spinotectal tract • Terminate in deep layers of superior colliculus. • For turning upper body, head and eyes in the direction of painful stimulus.
2nd order neuron: spinohypothalamic tract • Ascend to hypothalamus. • Associated with autonomic and reflex responses to nociception (e.g. endocrine and cardiovascular).
3rd order neurons –spinothalamic tract • Cell bodies in thalamus. • ventral posterior lateral, ventral posterior inferior and intralaminar thalamic nuclei. • Ventral posterior lateral nucleus gives fibres to posterior limb of internal capsule and corona radiata. Terminate in primary somatosensory cortex S-I (postcentral gyrus). Also sends fibres to secondary somatosensory cortex S-II.
3rd order neurons –spinothalamic tract • Ventral posterior inferior nucleus projects mostly to S-II but some to S-I. • Intralaminar nuclei projects to striatum (ie caudatae nucleus and putamen), S-I and S-II, cingulate gyrus and prefrontal cortex. • (Most nociception relaying fibres arriving at intralaminar nuclei transmit nociceptive information relayed there from reticular formation (have multiple synapses before arriving)).
3rd order neurons –spinoreticular tracts • Signals transmitted from reticular formation to intralaminar nuclei of thalamus, hypothalamus, limbic system. • Hypothalamus-autonomic and reflex. • Limbic-emotional/’suffering’.
Pain to face and head • Trigeminal nerve 3 branches: • Ophthalmic (V1) –scalp and forehead, upper eyelid, conjunctiva, cornea, nose, nasal mucosa, frontal sinus, meninges. • Maxillary (V2) –lower eyelid, cheeks, nares, upper lip, upper teeth/gums, nasal mucosa, palate and roof of pharynx, maxillary/ethmoid/sphenoid sinuses, meninges. • Mandibular (V3) – lower lip, lower teeth and gums, chin, and jaw (except angle), parts of external ear and meninges, mouth (not taste). • * V1 andV2 pure sensory, V3 mixed sensory and motor.
Pain to face and head • 1st order neuron carried by trigeminal nerve (cell body in Trigeminal/ Gasserian ganglion) enter pons, descend to medulla forming the spinal trigeminal tract and synapse in spinal trigeminal nucleus(caudal part) 2nd order neurons cross midline and ascend as trigeminothalamic tract VPM thalamus 3rd order neurons to sensory cortex
Primary somatosensory cortex S-I • Postcentral gyrus of parietal lobe • Brodmann’s areas 3a,3b,1,2. • Processing of pain localisation, intensity, quality, and sensory integration at conscious level. • Also sends signals to secondary somatosensory cortex.
Sensory homunculus • Downloaded from www.spinacare.wordpress.com.
Secondary somatosensory cortex S-II • At parietal operculum, ceiling of lateral sulcus. • Brodmann’s area 43. • Function in memory of sensory input and sensory integration.
Other brain areas related to pain • From electroencephalography (EEG), functional MRI (fMRI), magnetoencephalography (MEG), positron emission tomography (PET). • Anterior cingulate cortex (ACC), anterior insular cortex, supplemental area of motor cortex. • ACC and anterior insular cortices connected to limbic cortex.
Visceral pain • Visceral organs themselves have no pain receptors. Pain receptors embedded in walls of arteries serving these organs. • Diffuse, poorly localised, ‘referred’ to another somatic structure. • Nociceptive signals follow same pathway as signals from somatic structures. • Receptors: free nerve endings or Pacinian corpuscles. • First order neurons: C, Aδ or Aβ fibres. • Respond to stretching, or ischaemia. • Second order neurons: spinothalamic and spinoreticular tract.
Modulation of nociception • Gate control theory of pain • Impulses flow from periphery to brain through a ‘gate’ at spinal level. • Site at substantia gelatinosa (lamina II) where pain is modulated. • Small nerve fibers (C fibres) and large nerve fibers (Aβ fibres) synapse with: projection cells, which go up the spinothalamic tract to the brain, and inhibitory interneurons within the dorsal horn.
Descending pathway • Not as well understood as ascending one. • Originate at cortex, thalamus and brainstem (Periaqueductal grey; raphe nuclei and locus coeruleus). • Relay stations in brainstem. • Main neurotransmitters: noradrenaline, serotonin and endogenous opioids (enkephalin, beta-endorphin and dynorphin).
Descending pathway • PAG –main descending inhibitory control on the ‘gate’ mechanism in the dorsal horn. Has abundance opioid receptors and peptides. Connections with: • Nucleus raphe nucleus (serotonergic) inhibitory interneurones. • Locus coeruleus (Noradrenergic) dorsal horn.
Pain pathway in labour • Stage 1 labour (pain poorly localised) • Due to uterine (visceral) contractions and stretching cervix. • Sensation carried by mainly C-fibresinferior, middle and superior hypogastric plexus travel with sympatheticchain associated with dorsal rami of T10-L1 spinal nervesreferred visceral pain.
Pain pathway in labour • 2nd stage labour (pain sharp) • direct pressure by the presenting part on vagina and perineum • Stimulation of pudendal nerve (S2-4). • Aδ fibres carry impulse via pudendal nerve (S2-4) spinothalamic tract somatosensory cortex.
Pain pathway in labour • Other pain sensitive structures in the pelvis are also involved, i.e. the adnexi, the pelvic parietal peritoneum, bladder, urethra, rectum and the roots of the lumbar plexus. • Therefore L2 to S5 must also be blocked. There is an overlap and pain relief is not a simple matter of blocking T10 to L1 for the first stage and S2, 3, 4 for the second stage of labour.
Caesarean section • Higher block level (T4) due to peritoneal manipulation.
Pain pathway cornea • Cornea long ciliary nerves (also has sympathetic fibres) and short ciliary nerves (also has parasympathetic fibres +/- sympathetic)nasociliary nerve ophthalmic division trigeminal nerve (V1) (cell body in Trigeminal/ Gasserian ganglion) enter pons, descend to medulla forming the spinal trigeminal tract and synapse in spinal trigeminal nucleus(caudal part) 2nd order neurons cross midline and ascend as trigeminothalamic tract VPM thalamus 3rd order neurons to sensory cortex • *note sensory to conjunctiva:lacrimal branch V1 , vision:optic nerve.
Pain pathway -Cornea • Taken from Grey’s Anatomy.