Download
1 / 52
550 likes | 741 Views
Back Pain. Christopher D. Sturm, M.D., F.A.C.S Medical Director Mercy Institute of Neuroscience & Mercy Regional Neurosurgery Center. Back Pain. Extremely common Often accompanied by leg pain or numbness Adversely affects quality of life Lost time, work & money

E N D
Back Pain Christopher D. Sturm, M.D., F.A.C.S Medical Director Mercy Institute of Neuroscience & Mercy Regional Neurosurgery Center
Back Pain • Extremely common • Often accompanied by leg pain or numbness • Adversely affects quality of life • Lost time, work & money • Can vary in intensity and duration, leading to significant frustration
Back Pain But……THERE IS HOPE! You Do NOT have to just “live with it”
Back Pain • Can lead to nerve damage • Permanent loss of some functions • Movement • Sensory • Bowel and Bladder control • In some instances earlier treatment can lead to better outcomes
What to Do? • “So, what the heck is going on?” • “Can anything be done to fix it?” • “What are my options?” • “When should I start?” • “What are the success rates?”
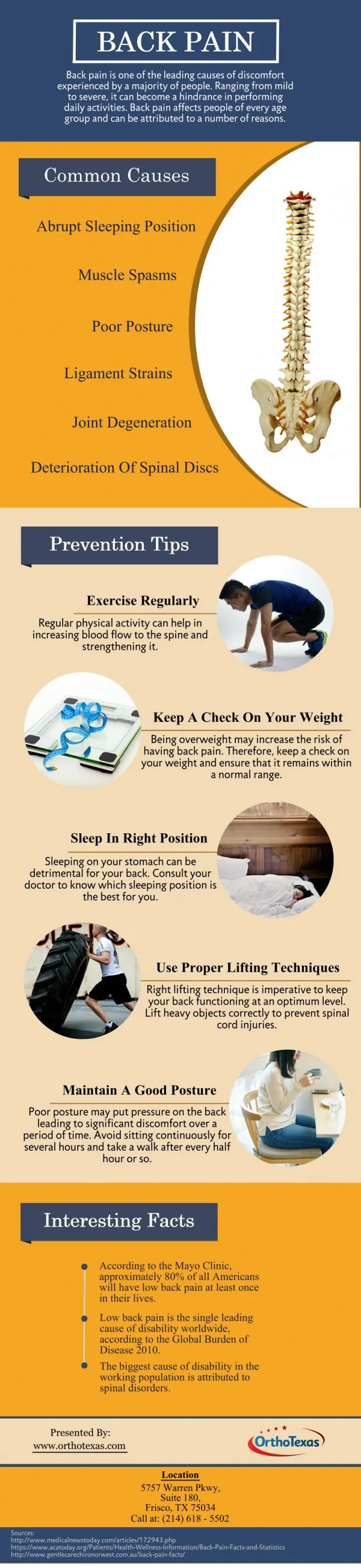
Causes of Back Pain • Muscle spasm/inflammation/strain • Degeneration or inflammation of the disc • Degeneration or inflammation of the back (facet) joints • Loss of normal alignment or instability • Fracture • Infection • Tumor
Evaluation of Back Pain/Leg Pain • Symptom history and physical exam findings • What makes it worse or better? • Location? • Duration? • Associated pain/numbness/weakness? • Bowel and bladder control? • Past medical history?
Evaluation of Back Pain/Leg Pain • MRI imaging • Optimal to evaluate discs, nerves, alignment • CT scan • Better visualization of the bone • Plain X-rays • Screening test • Bone Density study • Osteopenia/osteoporosis?
“So, what to do?” • Depends on the cause of the pain • Is there any associated loss of function? • Are the symptoms significantly interfering with your quality of life? • Any indication they are getting better? • Have conservative therapies failed?
Conservative Therapy • Symptom improvement without surgery • Activity modification • Pain medication • Physical therapy • Chiropractic intervention • Injectional therapy
When is Surgery Appropriate? • If the symptoms are significantly interfering with your quality of life, and have not improved with conservative therapy measures, for an appropriate period of time • Any presence, or high risk of functional loss • Instability • Tumor • Infection
Advancements in Spine • Improved imaging techniques • Pathophysiology of degenerative disease • Biomechanical advancements • Image guidance • Minimally Invasive techniques • Mechanical implantation devices
Mercy Regional Neurosurgery Multi-Center National Studies • CODA study • Posterior lumbar fusions • In-Fix study • Anterior lumbar fusions • Fortitude study • Cervical discectomy and fusions
Lumbar Degenerative Disease • Initial desiccation of the disc • Loss of structural integrity of the disc • Loss of disc space height/potential HNP • Abnormal loading and laxity of the facet joints • Neuroforaminal compromise • Malalignment and abnormal motion
Surgical Options • Lumbar discectomy • Lumbar laminectomy • Anterior lumbar interbody fusion (ALIF) • Posterior lumbar interbody fusion (PLIF) • Vertebroplasty/Kyphoplasty
Lumbar Discectomy • Leg pain unresponsive to conservative therapy • Progressive deficit • Cauda equina syndrome • Small incision • Outpatient or next day discharge
Lumbar laminectomy • Leg pain secondary to lumbar stenosis/lateral recess stenosis • Failure of conservative therapy • Older patients, slightly larger incision, longer stay • Approximate 10% incidence of subsequent lumbar instability
Anterior Lumbar Interbody Fusion (ALIF) • Lumbar degenerative disc disease producing mechanical LBP & minimal radicular pain • Localized concordant discogenic pain with discography at level(s) abnormal on MRI • Anterior approach avoids injury to posterior lumbar musculature • Suboptimal to address neural compression
L4-5 ALIF • 37 year old female with progressive mechanical LBP • Right leg psuedoradicular pain • Concordant L4-5 discogenic pain • Failed conservative therapy
Posterior Lumbar Interbody Fusion (PLIF) • Mechanical LBP with associated radicular pain and/or neurological deficit • Degenerative disc disease/collapse/herniation • Facet joint hypertrophy with foraminal stenosis • Lateral recess and/or central spinal stenosis • Spondylolysis/spondylolisthesis • Lumbar instability
L4-5, L5-S1 PLIF • 50 year old female with progressive LBP and bilateral radicular pain w/dysesthesia • Intensifying pain despite previous L4-5 hemilaminectomy/discectomy • Lumbar MRI – L4-5, L5-S1 DDD & NFS • Concordant discogenic pain L4-5, L5-S1
L5-S1 PLIF • 49 year old female with progressive LBP and left leg radicular pain • Dysesthesia left leg/foot • MRI – L5-S1 DDD with left NFS • Failed conservative therapy • Concordant discogenic pain L5-S1
Minimally Invasive Spine Surgery • Achieve same goals as “open” procedures • Smaller incisions • Less muscle trauma • Utilization of image guidance • Less post-operative pain • Shorter hospitalization
Results • Review of 5 years of practice data • Using the treatment approach outlined here • Improved or not? • Fusion? • Approximately 500 surgery patients • 93% reported improvement as a result of their surgery • 99% fusion rate
ACDF C4-5, C5-6 • 47 year old right handed female with posterior cervical pain and right arm radicular pain • Right deltoid and biceps weakness • Failed conservative therapy • Cervical spondylosis C4-5, C5-6