Download
1 / 32
380 likes | 1k Views
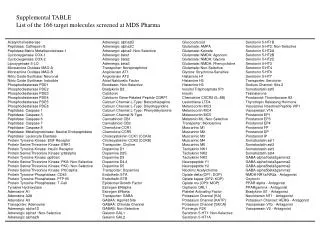
Alpha-adrenergic drugs. J. Starkopf Department of Anaesthesiology and Intensive Care University of Tartu Estonia. Alpha-adrenergic drugs. Content of the lecture: Adrenoreceptors Cellular mechanism of muscle contraction Catecholamines Autonomic nervous system Sympathomimetic drugs

E N D
Alpha-adrenergic drugs J. Starkopf Department of Anaesthesiology and Intensive Care University of Tartu Estonia
Alpha-adrenergic drugs Content of the lecture: • Adrenoreceptors • Cellular mechanism of muscle contraction • Catecholamines • Autonomic nervous system • Sympathomimetic drugs • Sympatholytic drugs • Clinical use
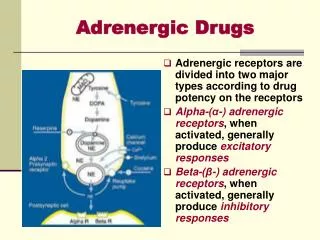
Adrenoreceptors Adrenoreceptors 1948 Ahlquist a and b adrenoreceptors 1967 Lands et al. b1 ja b2 1970 a1 and a2 , b1 and b2
Adrenoreceptors Adrenoreceptors
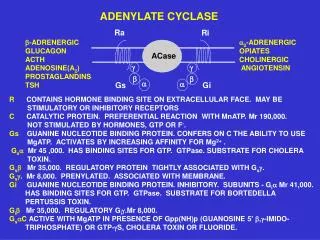
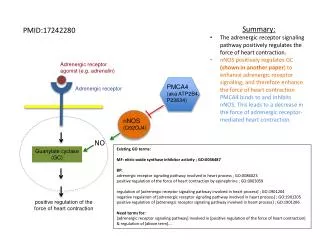
Cellular mechanisms of muscle contraction cAMP 5´AMP ATP phosphodiesterase Protein kinase A Ca2+ Ca2+ Ca2+ IP3 DAG Protein kinase C PIP2 Cardiomyocyte b1 Gs Adenylate cyclase Lusitropic effect Phospholamban Ca-pump Ca-channel Inotropic effect Gq Phospholipase C a1
Cellular mechanisms of muscle contraction Blood vessels • Vasoconstriction: • Symphatic nerve endings • Circulating catecholamines • Angiotensin • Endothelin • Vasodilatation: • Tissue metabolism • Cell depolarization • Endotheluim derived factors • NO • Prostacyclin • Bradykinin • Acetylcholine • Histamine
Cellular mechanisms of muscle contraction cAMP ATP Vascular smooth muscle cell ATII a1 b2 Gq Adenylate cyclase Gs Phospholipase C ET IP3 Protein kinase A Ca2+ Ca-pump Ca2+ Ca2+ Ca2+ + Calmoduline Myosine light chain kinase Vasoconstriction Vasodilatation
Autonomic nervous system • Nervous and humoral mechanisms which modify the function of the autonomous or automatic organs. • Innervation of smooth muscles, heart, endocrine glands. • Sympathetic nervous system • Parasympathetic nervous system • Enteric nervous system
Autonomic nervous system Adrenergic-receptor differentiation ALPHA Heart Blood vessels Arteries Veins GI tract Genitourinary tract Metabolic and endocrine effects BETA Heart Blood vessels Veins Respiration Metabolic and endocrine effects (1) Vasoconstriction (skin, gut, kidney, liver, heart) (2) Vasoconstriction (1) Sphincters (1) Contraction of sphincters, contraction of uterus (2) Deacreased insulin realease from pancreas (1) Increased rate and force of contraction (2) Vasodilatation (skeletal muscle, heart, brain) (2) Bronchodilatation (2) Glycogenolysis (muscle, liver) (1) Lipolysis (2) Gluconeogenesis
Autonomic nervous system Adrenoreceptors in the heart • Cardiomyocytes b1>>a1 • Sinus node b1=b2 • Coronary vessels a, b2 • b1 – positive inotropic and lusitropic effect • In normal heart: 77% b123 % b2 • Chronic heart failure: 60% b138 % b2 +a1
Sympathomimetic drugs Catecholamines Endogenous: • Adrenaline • Noradenaline • Dopamine Synthetic: • Isoprenaline • Dobutamine • Dopexamine Non-catecholamines Acting via adrenergic receptors: • Ephedrine • Phenylephrine • Methoxamine • Metaraminol Acting via non-adrenergic mechanisms: • PDE-inhibitors • others
Endogenous catecholamines Adrenaline Drug of choice for: Cardiac arrest Acute allergic (anaphylactic) reactions Occasionally as a bronchodilatator I/v in emergency situations; bolus – i/v infusion S/c – slower release due to local vasospasm
Endogenous catecholamines Adrenaline Dose: • Cardiac arrest 1 mg i/v (2…3 mg intratracheally) • Acute anaphylactic reactions 100 mg …1 mg i/v • Shock 0.01…0.2 mg/kg/min Cardiovascular effects on i/v infusion: • Low dosage: b2 effect – vasodilatation of skeletal muscle and splanchic arterioles. MAP remains stable • Higher dosage: a1, b1effects – vasoconstriction (incl. renal), increase in blood pressure and cardiac output, tachycardia
Endogenous catecholamines Adrenaline Other effects: • Metabolic effect • Hyperglycaemia • Potassium shift (hypokalaemia) • b2 stimulation drives K+ into red blood cells and muscle cells • Mydriasis • a1 effect; after CPR • Hypertermia in neonates
Endogenous catecholamines Noradrenaline • Arteriolar and venous vasoconstrictor • Acts almost exclusively at a-receptors • Infusion 0.01…0.1 (…1.0) mg/kg/min • Increase in systemic and pulmonary artery pressure • No effect on heart rate • No change in cardiac output • Renal vasoconstriction • Main indication: septic shock • Low systemic vascular resistance
Endogenous catecholamines Noradrenaline NB! Hypovolemia cannot be treated with noradrenaline!
Endogenous catecholamines Dopamine Stimulates: • DA1-receptors in renal and mesenteric arteries • a- and b-adrenoreceptors • Overall effect is related to the dose …3 mg/kg/min Renal and mesenteric vascular resistance, blood flow, glomerular filtration rate, diuretic effect 5…10 mg/kg/min b-mediated inotropic action, no vasoconstriction. Increase in CO and arterial pressure. Tachyarythmias. 10…15 mg/kg/min a-effect, similar to noradrenaline
Endogenous catecholamines Dopamine …3 mg/kg/min DA1 5…10 mg/kg/min b 10…15 mg/kg/min a
Endogenous catecholamines Vasopressors in septic shock Some advantages of norepinephrine and dopamine: • over epinephrine • potential tachycardia • possibly disadvantageous effects on splanchnic circulation • over phenylephrine • decrease in stroke volume Norepinephrine is more potent than dopamine and may be more effective at reversing hypotension. Dopamine may be particularly useful in patients with compromised systolic function but causes more tachycardia and may be more arrhythmogenic.
Synthetic catecholamines Synthetic cathecholamines Isoproterenol • b1and b2-agonist, with no a-activity • Heart rate, vascular resistance, cardiac output , arterial pressure • Treatment of bradyarrhytmias Dobutamine • b1agonist, moderate b2-agonist and mild a1-activity • Dose: 2.5…25 mg/kg/min • Cardiac output, vascular resistance, arterial pressure • Tachycardia Dopexamine • b2-agonist and DA1-agonist , moderate • Dose: 0.5…6.0 mg/kg/min • Heart rate , Cardiac output, vascular resistance, • Maintenance of splanchnic blood flow
Non-catecholamines Ephedrine • Similar effects as adrenaline • Agonist at a, b1and b2-receptors • Heart rate, arterial pressure • Dosage: • 5…15 mg i/v bolus • 15…30 mg i/m • Useful to treat hypotension • Induced by sympathetic blockade during regional anaesthesia • From general anaesthesia
Non-catecholamines Phenylephrine • Direct acting a1-agonist • Minimal agonist effects at a2 and b-receptors • Vasoconstriction, arterial pressure, heart rate • Dosage: • 50…100 mg i/v bolus (standard dilution 1:100) • 20…50 mg/min infusion • Useful to treat hypotension • From general anaesthesia
Sympatholytic drugs Drugs, which antagonize the effects of the sympathetic nervous system. They may act at • Central adrenergic neurones • a2-receptor agonists • Peripheral autonomic ganglia or neurones • Ganglion blocking drugs (e.g. hexamethonium) • Postsynaptic a- or b-receptors • a-blockers • b-blockers
Sympatholytic drugs Clonidine • a2-receptor agonist, a2: a1 > 200:1 • Stimulation of brain-stem a2-receptors decreases sympathetic tone • Arterial pressure, cardiac output • Synergistic analgesic effect with opioids • Treatment of delirium • Dosage: • 50…100 mg i/v bolus • 2 mg/kg/h infusion
Sympatholytic drugs Alpha-adrenergic antagonists Vasodilatators, used for treatment of hypertension or as urinary tract smooth muscle relaxants in patients with benign prostata hyperplasia Phenoxybenzamine • a1-receptor antagonist, a1: a2 > 200:1 • Long half-life • Preoperative preparation of phaeochromocytoma patients (chemical sympathectomy) Phentolamine Prazosin (Minipress)
Sympatholytic drugs Alpha-adrenergic antagonists Labetalol • a1-, b1- and b2-antagonist • Antihypertensive • Dosage: • 5…10 mg i/v bolus • …. infusion
Clinical use Standards! • Arterial line • Central venous line, whenever possible • Dilution of the drugs - standard dose regimens • Central hemodynamic monitoring if indicated