Download
1 / 56
571 likes | 598 Views
Chapter 13 Drugs Affecting Adrenergic Function. Question. The sympathetic nervous system produces what type of response? A. Adrenergic B. Antiadrenergic C. Cholinergic D. Anticholinergic. Answer. The sympathetic nervous system produces what type of response? A. Adrenergic

E N D
Question • The sympathetic nervous system produces what type of response? • A. Adrenergic • B. Antiadrenergic • C. Cholinergic • D. Anticholinergic
Answer • The sympathetic nervous system produces what type of response? • A. Adrenergic • The sympathetic nervous system produces an adrenergic response, and the parasympathetic nervous system produces a cholinergic response.
Chapter Summary • The nervous system is divided into two main branches, the central nervous system (CNS) and the peripheral nervous system (PNS). • The efferent division has neurons that carry signals away from the brain and spinal cord to the periphery. • The afferent division contains neurons that carry impulses from the periphery to the CNS. • The autonomic nervous system (ANS) is in turn subdivided into the sympathetic nervous system (SNS) and the parasympathetic nervous system (PSNS).
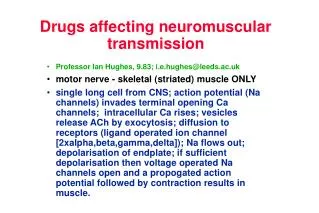
Function of the Autonomic Nervous System • The ANS has been identified as an involuntary system responsible for the control of smooth muscle. • The actual connection between neurons and effector organs or tissues relies on neurotransmitters and synaptic transmission. • The neurotransmitters in the ANS include acetylcholine (ACh), norepinephrine (NE), and epinephrine (Epi). • Synaptic transmission initially involves the synthesis of neurotransmitters in the nerve terminal. • In the SNS, preganglionic transmission is mediated by ACh, whereas postganglionic transmission is mediated by NE.
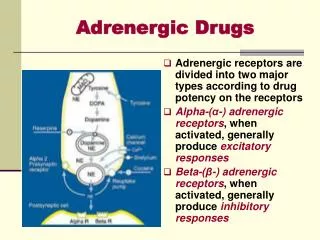
Adrenergic Receptors • In the SNS, there are several types of adrenergic receptors, including alpha-adrenergic and beta-adrenergic receptors. • Another type of receptor, the dopaminergic receptor, is related to adrenergic receptors in that dopamine is the precursor to NE. • Alpha and beta receptors are located throughtout the body. • Alpha-1 and beta-1 receptors respond to epinephrine, NE, and dopamine. • Alpha-2 receptors respond to epinephrine and NE. • Beta-2 receptors respond only to epinephrine.
Pathophysiology • The therapeutic uses of sympathetic drugs are related to providing extra-adrenergic stimulation or blockade of normal ANS functioning. • One of the most frequent indications for adrenergic agonist drugs is shock. • Shock is the result of inadequate tissue perfusion, leaving the cells without the oxygen and nutrients they need to function normally and survive.
Adrenergic Agonists • Adrenergic agonists are drugs that mimic the action of the SNS. • They exert their effects by direct or indirect stimulation of adrenergic receptors. • These drugs are generally divided into two groups: catecholamines and noncatecholamines. • Adrenergic agonists are also classified according to their selectivity. • Nonselective adrenergic agonists stimulate both alpha and beta receptors. • Prototype drug nonselective adrenergic agonist: epinephrine.
Epinephrine: Core Drug Knowledge • Pharmacotherapeutics • Wide variety of indications: asthma, shock, etc. • Pharmacokinetics • Administered: parenterally, topically, or by inhalation. Metabolism: liver. Absorption: into the tissues. Excreted: kidneys. Duration: 1-4 hours. • Pharmacodynamics • It stimulates all adrenergic receptors and causes adverse effects in the cardiovascular system and CNS.
Epinephrine: Core Drug Knowledge • Contraindications and precautions • Absolute contraindications to epinephrine include hypersensitivity, sulfite sensitivity, closed-angle glaucoma, and its use during labor. • Adverse effects • Severe adverse effects include hypertensive crisis, angina, cerebral hemorrhage, and cardiac arrhythmias. • Drug interactions • Tricyclic antidepressants, oxytocics, halogenated anesthetics, and beta blockers
Epinephrine: Core Patient Variables • Health status • Document preadministration vital signs. Review health history. • Life span and gender • Pregnancy risk category C • Lifestyle, diet, and habits • Document the patient’s occupation and daily activities. • Environment • IV administration only by trained personnel
Epinephrine: Nursing Diagnoses and Outcomes • Imbalanced Nutrition: Less Than Body Requirements related to drug-induced anorexia or nausea • Desired outcome: the patient will maintain adequate nutrition. • Disturbed Sleep Pattern, Insomnia, related to CNS excitation • Desired outcome: the patient will learn about and practice sleep hygiene. • Disturbed Sensory Perception related to impaired vision • Desired outcome: the patient will notify the provider if vision changes occur. • Ineffective Tissue Perfusion (Cardiopulmonary) related to cardiovascular effects of epinephrine • Desired outcome: the patient will notify the provider if tachycardia, chest pain, or palpitations occur.
Epinephrine: Planning & Interventions • Maximizing therapeutic effects • Requires close monitoring of vital signs and careful monitoring for adverse effects. • Take as prescribed. • Minimizing adverse effects • When treating anaphylactic shock, monitor blood pressure. • Assisting the patient with menu planning may help to promote appetite and counteract the anorectic influence of epinephrine.
Epinephrine: Teaching, Assessment & Evaluations • Patient and family education • Acute illness: Teaching should be brief, simple, and supportive. • Explain how to administer drug properly. • Ongoing assessment and evaluation • Assess the patient for resolution of the presenting problem. • Important to remember that epinephrine is a nonselective adrenergic agonist.
Question • Which of the following receptors is (are) stimulated by epinephrine? • A. Alpha 1 • B. Alpha 2 • C. Beta 1 • D. Beta 2 • E. All of the above
Answer • Which of the following receptors is (are) stimulated by epinephrine? • E. All of the above • Epinephrine is a nonselective adrenergic agonist. This drug stimulates alpha-1, alpha-2, beta-1, and beta-2 receptors. The only adrenergic receptor subtype it does not stimulate is the dopamine receptor.
Alpha-1 Adrenergic Agonists • The alpha-1 adrenergic agonists are drugs that stimulate the alpha-1 receptor directly. • Prototype drug: phenylephrine (Allerest)
Phenylephrine: Core Drug Knowledge • Pharmacotherapeutics • Used parenterally for vascular failure in shock. • Used topically for relief of nasal mucosal congestion. • Pharmacokinetics • Administered: parenterally or topically. Metabolism: liver. Excreted: urine. Onset: 15 to 20 minutes. Duration: 1-2 hours. • Pharmacodynamics • Is structurally similar to epinephrine and is a powerful alpha-1 adrenergic agonist.
Phenylephrine: Core Drug Knowledge • Contraindications and precautions • Hypersensitivity, sulfite sensitivity, severe hypertension, ventricular tachycardia, and closed-angle glaucoma • Adverse effects • Headache, restlessness, excitability, and reflex bradycardia • Drug interactions • Monoamine oxidase inhibitors (MAOIs), tricyclic antidepressants, and oxytocics
Phenylephrine: Core Patient Variables • Health status • Assess medical history and obtain baseline assessment • Life span and gender • Used in pregnancy only if absolutely necessary • Lifestyle, diet, and habits • Document the patient’s occupation and activities of daily living • Environment • Closely monitor during administration in acute care setting
Phenylephrine : Nursing Diagnoses and Outcomes • Impaired Gas Exchange related to bronchoconstriction • Desired outcome: gas exchange will remain unimpaired. • Imbalanced Nutrition: Less Than Body Requirements related to anorexia or nausea • Desired outcome: the patient will take sufficient nourishment. • Disturbed Sleep Pattern, Insomnia, related to CNS excitation secondary to phenylephrine use • Desired outcome: the patient will maintain normal sleep patterns.
Phenylephrine: Planning & Interventions • Maximizing therapeutic effects • Corrected any blood losses prior to administration. • To produce optimal mydriasis, instill the ophthalmic form into the conjunctival cul-de-sac. • Minimizing adverse effects • IV administration is through a large vein. • Avoid driving at night because blurred vision can be hazardous.
Phenylephrine : Teaching, Assessment & Evaluations • Patient and family education • Stress the hazards associated with driving and operating heavy machinery. • Teach the patient about drug interactions. • Ongoing assessment and evaluation • Completing a detailed and thorough history and physical examination is essential for any patient anticipating long-term adrenergic drug therapy.
Alpha-2 & Beta-Adrenergic Agonists • Alpha-2 adrenergic agonists • Stimulation of alpha-2 receptors in the CNS decreases sympathetic outflow by inhibiting the release of norepinephrine. • Beta-adrenergic agonists • Beta-adrenergic agonists also mimic the action of the SNS. • Beta-adrenergic agonists are also labeled according to their selectivity. • Prototype: dopamine (Intropin).
Dopamine: Core Drug Knowledge • Pharmacotherapeutics • Used to correct the hemodynamic imbalances present in shock. • Pharmacokinetics • Distribution: throughout the tissues. Metabolism: kidney, liver, and plasma. Excreted: kidneys. Onset: 5 minutes. Duration: 10 minutes. • Pharmacodynamics • Stimulates alpha-1 and beta-1 receptors: increased cardiac output
Dopamine: Core Drug Knowledge • Contraindications and precautions • Pheochromocytoma, uncorrected tachyarrhythmias, and ventricular fibrillation • Adverse effects • Ectopic beats, nausea and vomiting, tachycardia, angina, palpitation, dyspnea, headache, hypotension, and vasoconstriction
Dopamine: Core Patient Variables • Health status • Assess medical history (chronic illness & allergies) • Life span and gender • Pregnancy category C drug • Environment • Administered only in acute care settings
Dopamine : Nursing Diagnoses and Outcomes • Risk for Ineffective Tissue Perfusion to Vital Organs related to drug effect • Desired outcome: the patient will maintain sufficient perfusion of vital organs to prevent serious damage. • Risk for Injury related to adverse effects of drug therapy • Desired outcome: adverse effects of drug therapy will not occur or will be minimized to prevent injury.
Dopamine: Planning & Interventions • Maximizing therapeutic effects • Administer using an infusion pump to regulate flow. • Titrate dose to desired effect. • Minimizing adverse effects • Follow the manufacturer’s instructions for dilution. • Monitor IV site. • Assess for disproportionate rise in diastolic blood pressure.
Dopamine: Teaching, Assessment & Evaluations • Patient and family education • If administered during a crisis, limited teaching occurs at that time. • Reassure the patient and family that the patient will be monitored closely during administration of the drug. • Ongoing assessment and evaluation • Treatment is effective if blood pressure stabilizes, urinary output returns to normal, and cardiac output returns to normal.
Question • Dopamine is administered by which route? • A. Oral • B. IM • C. IV • D. ET
Answer • Dopamine is administered by which route? • C. IV • Dopamine is given only via the IV route.
Dopaminergic Agonists • There are five types of dopamine receptors; only dopamine-1 (DA1) and dopamine-2 (DA2) receptors mediate responses in the adrenergic nervous system. • Stimulation of DA1 and DA2 receptors results in peripheral vasodilation. • Stimulating both receptors may have either complementary or opposing effects. • Prototype drug: fenoldopam (Corlopam)
Fenoldopam : Core Drug Knowledge • Pharmacotherapeutics • Short-term management of severe hypertension. • Pharmacokinetics • Administered: parenterally. Metabolism: by conjugation. Excreted: urine and feces. Steady state: 20 minutes. • Pharmacodynamics • It does not bind with DA2, alpha, or beta receptors. It provides rapid vasodilation to the coronary, renal, mesenteric, and peripheral arteries.
Fenoldopam : Core Drug Knowledge • Contraindications and precautions • Hypersensitivity to sulfites • Adverse effects • Symptomatic hypotension, tachycardia, abdominal or back pain, GI effects, sweating, and CNS effects, such as insomnia, dizziness, nervousness, or anxiety • Drug interactions • Beta blockers and diuretics
Fenoldopam : Core Patient Variables • Health status • Medical history and pre-administration physical assessment • Life span and gender • Pregnancy category B drug • Environment • Administered only in the acute care hospital setting
Fenoldopam : Nursing Diagnoses and Outcomes • Risk for Ineffective Tissue Perfusion related to hypotension, tachycardia, or increased intraocular pressure • Desired outcome: the patient will maintain adequate tissue perfusion throughout therapy. • Risk for Injury related to hypokalemia • Desired outcome: the patient will maintain a serum potassium level within normal limits throughout therapy.
Fenoldopam : Planning & Interventions • Maximizing therapeutic effects • Dilute with 0.9% sodium chloride or 5% dextrose. • The drug is administered using an infusion pump. • Titrate dose to effect. • Minimizing adverse effects • Visually inspect the drug ampule. • Start at low doses and titrate up to avoid reflex tachycardia. • Monitor vital signs during administration.
Fenoldopam : Teaching, Assessment & Evaluations • Patient and family education • Explain to the patient and family the rationale for the use. • Reassure the patient that close monitoring will be maintained throughout drug therapy. • Ongoing assessment and evaluation • Monitor vital signs throughout infusion. • Evaluate the efficacy by monitoring blood pressure.
Alpha-Adrenergic Antagonists • Alpha-adrenergic antagonists block the stimulation of alpha receptors. • Alpha-1a receptors mediate human prostatic smooth muscle contraction. • Alpha-1b and alpha-1d receptors are involved in vascular smooth muscle contraction. • Prototype drug: prazosin (Minipress).
Prazosin: Core Drug Knowledge • Pharmacotherapeutics • Used to treat congestive heart failure, Raynaud vasospasm, and prostatic outflow obstruction. • Pharmacokinetics • Administered: oral. Metabolism: liver. Excreted: bile, feces, and urine. Onset: 1 hour. Duration: 10 hours. • Pharmacodynamics • Blocks postsynaptic alpha-1 adrenergic receptors: lowers supine and standing blood pressure.
Prazosin: Core Drug Knowledge • Contraindications and precautions • Hypersensitivity; use caution with angina because hypotension may worsen the condition • Adverse effects • Light-headedness, dizziness, headache, drowsiness, weakness, lethargy, nausea, and palpitations • Drug interactions • Other antihypertensive medications
Prazosin: Core Patient Variables • Health status • Past medical history and physical assessment • Life span and gender • Pregnancy category C • Lifestyle, diet, and habits • Document the occupation and daily activities • Environment • Assess environment where drug will be given
Prazosin: Nursing Diagnoses and Outcomes • Ineffective Tissue Perfusion related to prazosin-induced hypotension • Desired outcome: the patient will maintain adequate tissue perfusion. • Imbalanced Nutrition: Less Than Body Requirements related to nausea secondary to prazosin use • Desired outcome: the patient will receive adequate nourishment by practicing appropriate dietary management. • Risk for Injury related to orthostatic hypotension • Desired outcome: the patient will remain free of injury.
Prazosin: Planning & Interventions • Maximizing therapeutic effects • Take as prescribed. • Refraining from OTC medication usage. • Minimizing adverse effects • Take the first dose just before bedtime. • Monitor weight and check for edema.
Prazosin: Teaching, Assessment & Evaluations • Patient and family education • Take drug as prescribed. • Adverse effects, including symptoms, to report to doctor. • Ongoing assessment and evaluation • Monitor blood pressure, heart and lung sounds, and edema. • Identify potential drug interactions.
Beta-Adrenergic Antagonists • Grouped according to their specificity of action at the beta-1 and beta-2 receptors. • Stimulation of beta-1 only (tachycardia, increased lipolysis, inotropy). • Stimulation of both beta-1 and beta-2 receptors (vasodilation, decreased peripheral resistance, bronchodilation). • Prototype drug: metoprolol (Lopressor, Toprol XL).
Metoprolol: Core Drug Knowledge • Pharmacotherapeutics • Treatment of hypertension, angina, and controlled congestive heart failure. • Pharmacokinetics • Administered: parenterally and orally. Metabolism: liver. Excreted: urine and breast milk. Onset & duration: varies with route of administration. • Pharmacodynamics • Decreased cardiac output and blood pressure. • Slowing of atrioventricular conduction and suppression of automaticity.