Download
1 / 21
210 likes | 674 Views
Fractures of the Pelvis and sacrum. By Sarah Hansen SPTA. Objectives. Be able to list and differentiate between the different classification systems for pelvic fractures. Demonstrate knowledge of the classification systems for sacral fractures.

E N D
Fractures of the Pelvis and sacrum By Sarah Hansen SPTA
Objectives • Be able to list and differentiate between the different classification systems for pelvic fractures. • Demonstrate knowledge of the classification systems for sacral fractures. • Be able to apply the terms and information from this in-service to everyday chart reviews, documentation, and pt treatments.
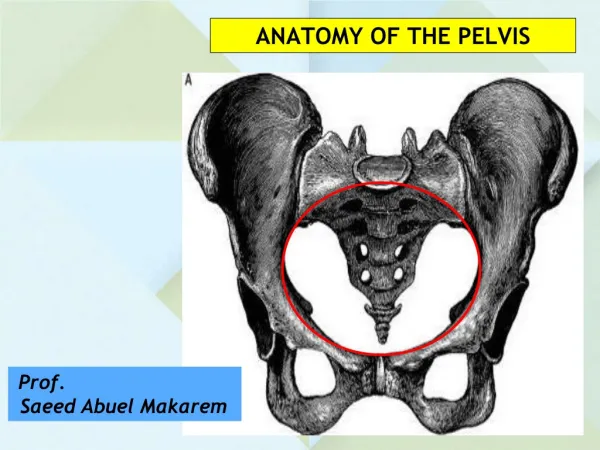
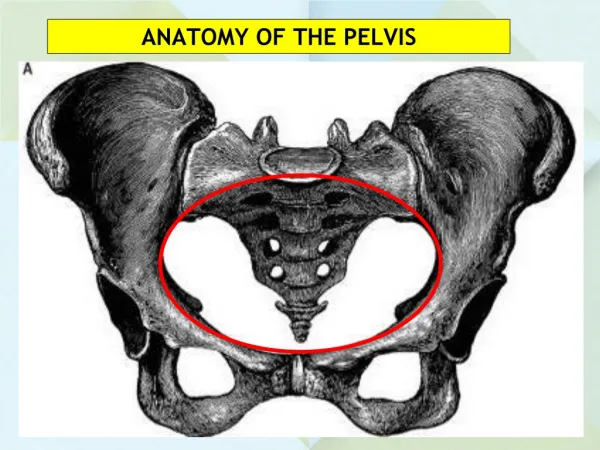
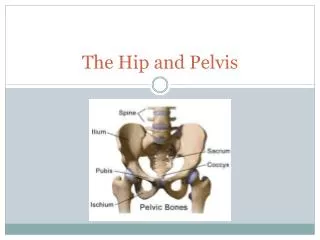
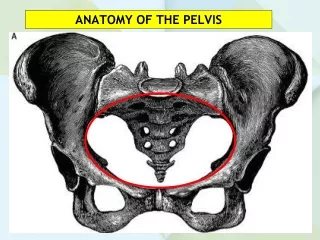
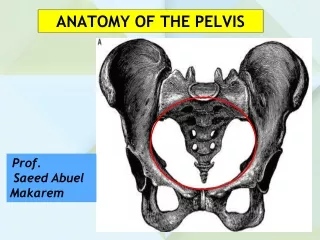
Bones of the pelvis: Ilium Ischium Pubis Tri-radiate cartliage Acetabulum
Cont… • The acetabulum is formed around the cartilaginous junction of the three pelvic bones, the ilium, ischium, and pubis. • This junction is called the tri-radiate cartilage, it is a Y-shaped synchondrosis centered on the acetabulum. • Complete fusion of the innominate bone occurs in the late teens.
Pelvic Fx classification • There are two commonly used classification systems for pelvic fractures: -Letournel and Judet -Young Burgess
Letournel and Judet:Columns Anterior column (aka iliopubic column) Posterior column (aka ilioischial column)
Columns of the pelvis: • From the lateral view, the tri-radiate cartilage junction resembles a Y with the longer limb forming the anterior column and the shorter, the posterior column of the acetabulum. • These columns transfer forces from the lower extremities through the hip and sacroiliac joint into the axial skeleton.
Letournel and Judet: Ant./Post. Injuries Injuries to the anterior column usually occur when forces are applied to the hip in external rotation. Injuries to the posterior column usually occur when forces are applied to the hip in internal rotation.
Letournel and Judet:Pelvic fx classification Description: Treatment: Anterior column May compromise any May require screws and portion of ant column. Plates to stabalizefx. Anterior wall Involves central portion of Reduction/internal fixation ant column. Anterior column Involves ant wall fx Reduction/internal fixation posterior transverse and post. Transverse fx
Letournel and Judet:Pelvic fx classification Description: Treatment: Posterior column Often result of MVA, Internal fixation usually dashboard impact. Sciatic nerve commonly inj. Posterior wall Most common pelvic fx ORIF Involves central part of posterior column. Posterior column Multiple fxs in posterior Internal fixation, Posterior wall column of pelvis. Immediate surgery
Letournel and Judet:Pelvic fx classification Description: Treatment: Transverse Both ant/post columns Screws/plates, ORIF are broken. Both column both ant/post columns ORIF are broken in a more vertical orientation. Transverse Usually caused by a blow Posterior wall directly upon the gr. trochanter. T-shape Poorest clinical results.
Young Burgess: Anterior Posterior Compression (APC) Description: Treatment: APC ISymphysis widening < 2.5 cm. Non-operative. Protected WB APC II Symphysis widening > 2.5 cm. Anterior symphyseal Anterior SI joint diastasis. plate or ext fixator. Posterior SI ligaments intact. APC III Disruption of ant/post Anterior symphyseal plate or SI ligaments (SI dislocation). external fixator. posterior Associated with vascular injury. stabilization with SI screws.
Young Burgess: Lateral Compression (LC) Description: Treatment: LC I Oblique ramus fracture and Non-operative. ipsilateral anterior sacral Protected WB. compression fracture. LC IIRamii fracture and ipsilateral Open reduction and posterior ilium fracture dislocation internal fixation of ilium. (Crescent fracture). LC III Ipsilateral lateral compression and Posterior stabilization with contralateral APC (windswept pelvis). plate or SI screws Common mechanism: rollover MVA or as needed. pedestrian vs auto.
Young Burgess:Vertical Shear (VS) Description: Treatment: Vertical shear (VS) Posterior and superior directed force. Posterior stabilization with Associated with the highest risk of plate or SI screws hypovolemic shock (63%); mortality as needed. rate up to 25%.
Other terms: Stable Unstable • Single fractures of the pelvic ring. • Pure acetabularfx, straddle fx, chip/avulsion fx. • Pelvic ring is disrupted in more than one location. • Posterior pelvis, sacrum, or sacroiliac complex is disrupted. • Malgaignefx • Bucket handle fx • Open book fx
Other terms: Straddle fx: Bilateral superior and inferior rami fractures. -Originally described in horseback riders. Chip/Avulsion fx: injury at a tendon/ligament attatchment. Where the tendon or ligament pulls off a piece of the bone. Malgaignefx: Two vertical fractures involving one side of the pelvic ring. -One anterior to acetabulum and one posterior.
Cont… Bucket Handle fx: Fracture of anterior arch and contralateral posterior arch. Usually caused by direct blow to pelvis, may cause rotary deformity of the hemipelvis that was effected as well as leg length discrepancy. Open Book fx: Separation of pubic symphysis
Sacral fractures:Denis Et Al Zone I - Fractures occur lateral to the sacral foramina. -The most common, accounting for 50% of the fractures in the series of Denis et al. -Zone-I fractures mainly involve the sacral ala, with possible extension into the sacroiliac joint. Neurological injury occurs in approximately 6% of patients and typically involves the L4 and L5 nerve roots. Zone II - Vertical transforaminal fracture without involvement of the sacral spinal canal. -Second most common pattern, accounting for 34% of sacral injuries. -Neurological injury is found in 28% of patients, and most frequently affects the L5, S1, or S2 nerve root.Malunionsin this area are associated with very poor functional outcomes. Vertical shear injuries are considered to be highly unstable zone-II fractures. Zone-III - Any sacral fracture involving the spinal canal. -Least frequently encountered fracture pattern, only 16%. -Zone III injuries are associated with the highest prevalence and severity of neurological injury, about 57%.
Other sacral fx classification Sacral Insufficiency Fracture: A stress fracture of the sacrum that is most common cause is postmenopausal osteoporosis, presents with groin, low back, and buttock pain. Transverse Fractures: -Upper (S1-S3): higher incidence of bladder dysfunction. -Lower (S4-S5): very unstable, require surgery to stabilize from sacrum to lower lumbar spine. U-shaped sacral fracture: -Results from axial loading and is associated with spino-pelvic dissociation. -Formed by bilateral transforaminal sacral fractures connected by a transverse fracture (usually between 2nd and 3rd segments). -High incidence of neurologic complications, usually involves a disruption of caudaequina at level of transverse fx.
Something to keep in mind… “Once reconstruction occurs, the next challenge is rehabilitation of the injured patient. Surgeons have become increasingly aware that outcome is not simply an x-ray finding, or even a score on a validated scale. Outcome for the patient with pelvic and acetabular injuries is a complex analysis that comes down to the basics of life for many patients. Posttraumatic arthrosis chronic pain, nerve damage and bowel, bladder, and sexual dysfunction, intertwined with psychological distress are the real challenges to the patient. No matter how heroic the initial work and salvage of the patient’s life, ultimately the quality of life becomes the sine qua non of a “good” result. While many centers are working diligently to improve the acute outcome of pelvic fracture patients and fixation techniques for the pelvis and acetabulum, the time has come to apply the same energy toward improvements in post-injury rehabilitation. The interface of the patient, the surgeon, the rehabilitation specialist, and society may be the next frontier in the management of pelvic and acetabular injuries.” http://www.scribd.com/doc/46866708/Fractures-of-the-Pelvis-and-Acetabulum
Bibliography: Denis, Francis M.D.; Davis, Steven B.S.; Comfort, Thomas M.D. Current Orthopaedic Practice. Sacral Fractures: An Important Problem Retrospective Analysis of 236 Cases. February 1988. Available at http://journals.lww.com/corr/abstract/1988/02000/sacral_fractures__an_important_problem.10.aspx. Accessed 9/26/12 PhiefferLS, Lundberg WP Templeman DC. PubMed. Instability of the posterior pelvic ring associated with disruption of the pubic symphysis. October 2004. Available at http://www.ncbi.nlm.nih.gov.dbprox.slcc.edu/pubmed/15363918. Accessed 9/12/2012. Routt ML Jr, Simonian PT. PubMed. Internal fixation of pelvic ring disruptions. 1996. Available at http://www.ncbi.nlm.nih.gov.dbprox.slcc.edu/pubmed/8915199. Accessed 9/12/2012 Scheterer MJ, Osterhoff G, Wehrle S, Wanner GA, SimmenHP,Werner CM. PubMed. Detection of posterior pelvic injuries in fractures of the pubic rami, June 6, 2012. Available athttp://www.ncbi.nlm.nih.gov.dbprox.slcc.edu/pubmed/22682148?dopt=AbstractPlus. Accessed 9/12/2012 Young JW, Resnik CS. PubMed. Fracture of the pelvis: Current concepts of classification. December 1990. Available at http://www.ajronline.org/content/155/6/1169.long. Accessed 9/12/2012.