Download
1 / 6
60 likes | 214 Views
C. difficile Subcommittee Summary HAI Advisory Committee Nov 18, 2010 Submitted by R. Murthy, MD (Subcommittee Chair). Activities of Subcommittee Sep-Oct. Reviewed published criteria for CDI reporting Followup with CDPH re CDC NHSN updates to CDI reporting options

E N D
C. difficile Subcommittee Summary HAI Advisory CommitteeNov 18, 2010Submitted by R. Murthy, MD(Subcommittee Chair)
Activities of Subcommittee Sep-Oct Reviewed published criteria for CDI reporting Followup with CDPH re CDC NHSN updates to CDI reporting options Recommendations for reporting of CDI data
Followup - NHSN • NHSN LabID module (modification to add elements requested) – CDPH followup • The facility testing method for C diff will be added and available with the next upgrade of the NHSN module sometime during first half of 2011 • A checkbox as requested for healthcare exposure other than facility will not be added BUT the use of a custom field is available for our use • Both of these fields would be voluntary and not mandatory • Action: Subcommittee to discuss further re use of custom fields for CA hospitals for stratification
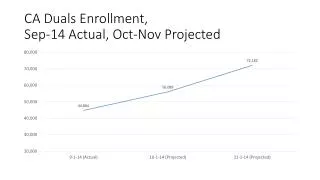
Recommendations • Jan 2011 reporting of CDI based on data reported by CA hospitals 2009-Mar2010 (paper submission) • Strong recommendation from group to that CDPH only report CDI data that was submitted by hospitals beginning April 2010 (when LabID method was implemented for hospital reporting) and not report prior data submitted on paper due to inability to compare among hospitals and validate accuracy of data). • For the Jan 2011 report, group recommends that CDPH defer reporting of CDI data until June 2011 when submitted data follows the same surveillance methods and CDPH has had an opportunity to validate data. The group recommends that CDPH list the hospitals that have submitted data for 2009-Mar 2010. • As an alternative, if pressed to report rates, the group recommends CDPH report a CDI rate for the State, which would include community-acquired, healthcare-acquired, or facility-acquired. This would allow for an estimate of the burden of CDI in CA overall to be described, while acknowledging that there are significant flaws with the reporting and that this rate is not comparable to any subsequent rates. This would also provide for the opportunity to prepare for the publication of rates that are more comparable using standard methodology by hospitals by introducing appropriate terminology and the guidance in understanding the issues related to CDI.
Recommendations (contd) • The following points are the basis for the above recommendations re data reported from 209-Mar 2010 • CDPH reported that the data submitted by hospitals on paper requires significant effort by CDPH to clear up prior to reporting (contacting hospitals for clarifications or corrections) • Methodology used by hospitals is inconsistent and not standardized and the type of diagnostic test used not considered (the traditional test may have false negative rates up to 25%) • Data from this time period would be very difficult to interpret let alone use for any meaningful comparison between hospitals • Not all hospitals have reported
Recommendations • Education information to provide for the website being prepared by the Public reporting subcommittee • Group discussed the importance of describing the terminology for the website – specifically information regarding Healthcare associated CDI and attribution of CDI. • Whenever a rate is linked to a healthcare facility, the consumer will attribute the rate to that healthcare facility. In the case of CDI, depending on the healthcare facility, a number of patients will have had prior contact with other healthcare venues, such as skilled nursing facilities, dialysis centers, infusion clinics, and still be would have been hospitalized within 30 days at that facility. • NHSN considers facility onset any case of CDI (ie lab test positive) that occurs in a patient who had been hospitalized within 30 days before the diagnosis, regardless of whether there has been contact with other healthcare facilities. • Recommendation: Therefore, it is critical until there is more refinement in the reporting to use the term “healthcare-associated” with the caveat that this rate could be attributed to facility, SNF etc