Download
1 / 17
170 likes | 200 Views
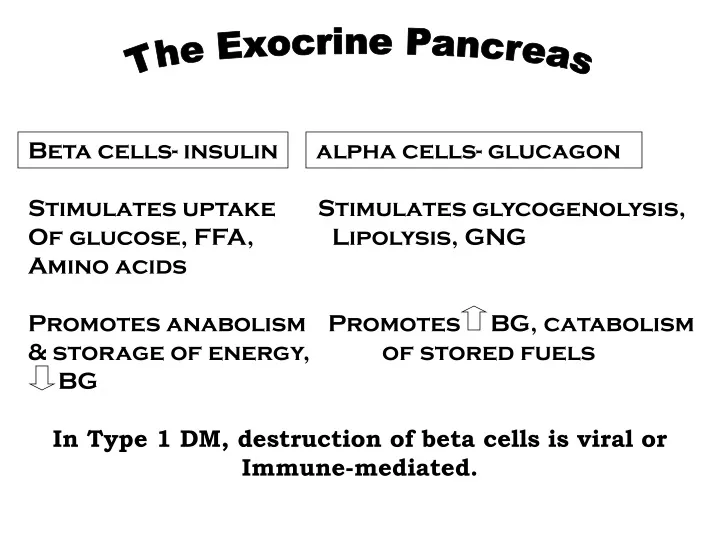
The Exocrine Pancreas. Beta cells- insulin alpha cells- glucagon Stimulates uptake Stimulates glycogenolysis, Of glucose, FFA, Lipolysis, GNG Amino acids Promotes anabolism Promotes BG, catabolism & storage of energy, of stored fuels BG.

E N D
The Exocrine Pancreas Beta cells- insulin alpha cells- glucagon Stimulates uptake Stimulates glycogenolysis, Of glucose, FFA, Lipolysis, GNG Amino acids Promotes anabolism Promotes BG, catabolism & storage of energy, of stored fuels BG In Type 1 DM, destruction of beta cells is viral or Immune-mediated.
Monitoring: Factors that affect Blood Glucose Levels Food Insulin Deficiency Stress Illness Infection Glucagon et al. Too much insulin or oral agents Not enough food Unusually high activity Skipped or delayed meals
Insulin Therapy Three Examples: Type I: Basal/ Bolus Regimen-- Lispro (Humalog)/NPH Premeal Humalog x 3 Bedtime NPH to control hyperglycemia at night (may need some NPH mixed with Humalog during the day to provide background insulin throughout the day) Split/Mixed NPH-Lispro Regimen NPH/Humalog mixtures at morning and late pm meals (~6 am & 6 pm) (provides enough NPH for bkgd coverage during the night)
Example 3: Type 2 DM BIDS (Bedtime Insulin-Daytime Oral Agent) Oral hypoglycemic medication(s) (e.g., sulfonylureas, etc.) to keep PG down during day. Bedtime NPH insulin to keep hepatic glucose production down during night. Starting dose= wt (#) / 10 150# / 10 = 15 units NPH at bedtime Increase 4-5 units/ wk until FPG < 140 mg/dl
Metabolic Effects of Exercise in Type 1 DM AdequateInsulin TrtInadequate Peripheral Glucose Uptake Hepatic Glucose Output Glucagon Production Blood Glucose
Frequency of Monitoring • American Diabetes Assn. Clinical Practice Recommendations (1998): - type 1: frequent SMBG (at least 3-4 x/ day) - type 2: daily for those trted with insulin, oral agents, or both Only use SMBG if a part of an integrated treatment program.
Monitoring: Goals 1. Achieve and maintain target BG levels. 2. Prevent and detect hypoglycemia. 3. Adjust medication (e.g., insulin) with with lifestyle changes (e.g., food and physical activity). 4. Serum Lipids, Blood Pressure, BMI
Monitoring: Implementation 1. Establish target BG ranges 2. Determine frequency of monitoring 3. Record results 4. Identify patterns so that medications meal plans physical activity can be adjusted.
Hypoglycemia and its Management Sx Mgmt Approaches Nervous Assess BG, if possible Headache Start with quick-acting CHO sources: Sweating glucose tabs or gel Weakness 1/2 c. sugar soft drink or juice Confusion 4-7 Lifesavers-type candy Tremors 1 c. of milk Lethargy Have a snack, unless before a meal Look for cause of hypoglycemia If an insulin user, inject glucagon.
Symptoms of Hyperglycemia Three Polys fatigue Glycosuria acetone breath Weight Loss Labored breathing (kussmaul respirations)
Physical Activity in Type 1 DM • Confers great benefits but requires good planning! • If BG <80 or > 300 = Don’t Exercise!! • BG varies widely even with small amounts of exercise. Depends on control level. • Check PG before exercise. If moderate activity, add 10-15 g CHO; if vigorous, add 20-30 g CHO. • Check PG 30 min. before and 1 hour after exercise.
Metabolic Effects of Exercise in Type 2 DM Lipolysis Decreased Plasma Insulin Lower Blood Glucose Increased peripheral glucose uptake Increased Insulin Sensitivity
Multiple Dose Regimen When Therapy Changes NPH + Humalog BID Add Bedtime NPH to Orals Combinations of Oral Agents: Metformin + Sulfonylureas, etc. Monotherapy Oral Agents: Sulfonylureas, Metformin, Troglitazones, etc. Meal Planning and Physical Activity
Evaluating Outcomes in DM Treatment Outcomes Can Be: Clinical Economic Quality of Life Glycemic Control length/stay Participation in HbA1c ER visits care Blood lipids costs to - SMBG Weight/BMI health plan - keeps appts. Blood pressure - Rx refills Complications Better work Q of Life survey attendance
Case Study: 12 y/o with Type 1 DM Yusef Pt presented with weight loss, polyuria, polydipsia Dx: Type 1 DM ER Visit post-Dx: N/V/ Thirst, Fever, High BG (~400) Confused, Acetone Breath Urine reveals glycosuria, ketonuria= DKA
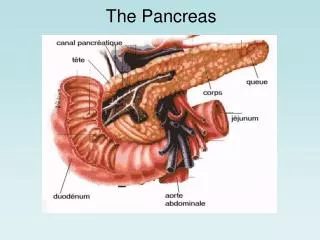
Metabolic events leading to these Sx?? Gradual Loss of Pancreatic Beta Cell Function Body loses major anabolic hormone= cells starve Cell starvation leads to increase glucagon, attempt to provide fuel to cell via gluconeogenesis. None of the fuel reaches the cell-urinary loss Extra water needed to clear glucose=polydipsia (thirst) Fat catabolized faster than used= ketone build-up
Symptoms of Diabetic Ketoacidosis Nausea Headache Dry, itchy skin Kussmaul Respiration Positive urinary ketones BG < 60 mg/ dl Gradual Onset of Symptoms