Download
1 / 26
300 likes | 520 Views
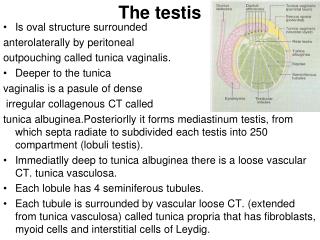
Testis. Often difficult to differentiate a serious emergent situation from a more benign situation Pay attention to history, clinical picture and pain expression of patient Decide who needs tests and when Decide who needs to go to surgery emergent and who elective.

E N D
Testis • Often difficult to differentiate a serious emergent situation from a more benign situation • Pay attention to history, clinical picture and pain expression of patient • Decide who needs tests and when • Decide who needs to go to surgery emergent and who elective
Scrotal Swelling Presentations HERNIA Hydrocele Scrotal abscess Varicocele TORSION Epididymitis
Hernia • Bulge over inguinal canal or scrotum • Changes size • Reducible • Sometimes there, sometimes not • Open processus vaginalis • Often not painful • Diagnosis by exam • Aggravated by constipation • Elective surgery unless incarcerated
Hydrocele • Bulge in scrotum or over inguinal canal • Changes size if communicating • Translucent • Diagnosis by exam • Elective surgery ..but starts screaming during exam Not painful
Torsion • 1 in 4000 males <25/year • Bell clapper deformity • Lack of fixation • Testis freely suspended within the tunica vaginal • Extravaginal • Pre- or neonatal • Intravaginal • Older children • Peak around 13 years • Left more common • 2% bilateral • Trauma as cause is rare • Only 4%-8% Barada et al, J Urol 1989 Seng et al , J Accid Emerg 2000
Sudden onset of extreme pain Followed by acute swelling Affected side elevated Nausea and emesis No cremasteric reflex Can present as abdominal pain!!! If pain gets better by itself Not good – NECROSIS!!! Diagnosis by exam and Doppler - Ultrasound Torsion NO FLOW Minevich E, emedicine Barada et al, J Urol 1989
Torsion - Treatment • Manuel de-torsion can be attempted • But extremely painful • “Open book” • Don’t delay diagnosis • Immediate surgery • Within 6 hours • Untwist and check for viability • Remove necrotic testis • Fixate the other side • Prevent future torsion
Torsion- Prenatal • Extravaginal torsion • Presentation at birth • Non-painful • Hard • Attached to scrotal wall • Dark color shines through scrotum • Treatment • Orchiectomy • Fixate contralateral side
Torsion • “Must not miss” diagnosis • Consider diagnosis until proven otherwise • Doppler Ultrasound • …but perform surgery even if studies are negative if clinical suspicion is high
Torsion Appendix testis • Painful • Swollen in upper part of testis • Blue dot sign • Difficult to differentiate from testicular torsion • Diagnosis by exam and ultrasound • Often found during exploration of testicular torsion • Surgery not necessary if clearly identified on US
Scrotal abscess • Many possibilities • Bug bite/ Rash • Orchitis/ Epididimytis • Trauma • Exotic infection • Immune disorder • Treatment • Antibiotics • Drainage • Debridment • Evaluate reason
Epididymitis/Orchitis • Very Painful • Onset gradually • Swollen and red • Epididymis more painful than testis • Diagnosis • Exam, Lymph nodes, US, UA • Infection • UTI (UTI pos) • Hematogenous (UA neg) • Reactive (UA neg) • Consider malformation • Ectopic ureter • Treatment • Antibiotics (E.coli –Bactrim) • Elevation • Cool Increased flow to the epididymis
Varicocele • Dilation of the pampiniform venous plexus and the internal spermatic vein • Typically left • insertion of vein into renal vein • If right or no decompression on exam US recommended to rule out intra abdominal process • Usually asymptomatic and found on routine exam • Typical exam- Bag of worms • Three reasons for OR • Pain • Cosmetic • Testicular dysfunction • US to verify diagnosis and measure testis Patient does not want to be here Redman et al, J Urol 2001, Sheldon et al, J Urol 2001
Testicular Tumors • 2% of all pediatric tumors • Incidence of 0.05-2 per 100,000 children • First peak in the first 2 years of life, second in young adulthood • Adult: • mostly germ-cell tumors with malignant potential (Seminoma and Embryonal carcinoma) • Prepubertal: • yolk-sac tumors (malignant) • Teratoma benign in children • Seminomas and mixed germ-cell tumors are extremely rare • Gonadoblastoma: associated with DSD • Leukemia • Paratesticular: Rhabdomyosarcoma
Testicular Tumors • Presentation • Painless scrotal swelling (85%) • Trauma, Hydrocele, Torsion • Diagnosis • Exam • Ultrasound • aFT (yolk-sac), bHCG (Gonadoblastoma), Testosteron (Leydig- cell tumor) • Excellent survival rates Cooper CS, Urol Oncol 2005
Testicular Tumors Surgery with radical orchiectomy in 24 hours after diagnosis
Cryptorchidism • Testis should descend from 7 months gestation until birth • About half of UDT will drop during first year • Can be intraabdominal, in canal or ectopic
Cryptorchidism • Exam can be difficult • Often strong cremasteric reflex • Differentiate between retractile and undescended • Frogleg and try to milk testis into scrotum • Consider ectopic position • Let the parents feel the testes Child comfortable…until exam
Cryptorchidism • Clinical diagnosis • Consider testicular atrophy if the other testis is large • Ultrasound, MRI, CT usually not helpful… • If testis is not palpable – OR • If testes is found on imaging – OR • If testes is not found on imaging – OR • Reason for surgery • Fertility • Self- examination to detect testis tumor • Timing of surgery: after 6 month gestational age
Female Genitalia • Labial adhesions • Fusion of labia minora • Not painful • No emergency • Can usually void fine • Treatment: • Lysis (NO!!) • Estrogen crème • Lysis under local or full anesthesia • Observation
Imperforate Hymen • Normal urethral opening • Bulging introitus • Can be opened in clinic • Not painful • Should be seen soon
Sexual abuse • Detailed knowledge of the anatomy • Differentiate normal from abnormal • Suspicious behavior during examination • Immediate contact of social services
Syndromes • Multiple syndromes impact the outer genitalia • Many detected prenatally • Should be referred for prenatal consultation • Immediate contact with center • Postnatal transfer to center • Inform parents that situation will be discussed in detail at the center
Syndromes - DSD • DSD PAIS (46XY) CAH Complete androgen insensitivity (CAIS) Genetic Male DSD
Syndromes - Exstrophy Bladder Exstrophy Cloacal Exstrophy