Download
1 / 37
390 likes | 645 Views
Tumors of the testis. KVB. Important facts about testicular tumors. Uncommon, incidence: 5/100,000 men <1% of all malignancies in men Peak: 30-40 years, rare in prepubertal children & elderly >90% are of germ cell origin >90% are malignant

E N D
Important facts about testicular tumors • Uncommon, incidence: 5/100,000 men • <1% of all malignancies in men • Peak: 30-40 years, rare in prepubertal children & elderly • >90% are of germ cell origin • >90% are malignant • Serum tumor markers found in 50% of patients. Eg: AFP, hCG
Risk factors for testicular cancers • Sex chromosome abnormalities: Germ cell tumors occur at a rate of 25% in dysgenetic gonads,intersexes, hermaphrodites & pseudohermaphrodites. • Cryptorchidism: 10-fold increase in incidence of testicular germ cell tumors.
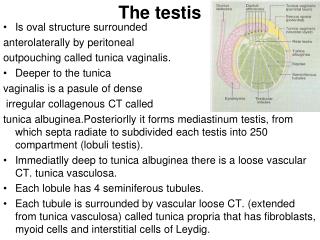
Histogenesis of testicular germ cell tumors • Originate from intratubular germ cells that have undergone malignant transformation • First occurs as carcinoma-in-situ or intratubular testicular germ cell neoplasia (ITTGCN) • Malignant cells have enlarged, hyperchromatic nuclei & cytoplasm filled with glycogen
ITTGCN is usually diagnosed incidentally during biopsy for infertility workup
Clinical classification of testicular tumors • Seminomas (40%) • Nonseminomatous germ cell tumors (NSGCT) (40%) • 15% of tumors have both seminomatous & nonseminomatous elements. • Nonseminomatous elements are more malignant, therefore such tumors are clinically treated as NSGCT.
Seminoma • Most common type of germinal tumor (50%) • Most patients are 25-45 years of age • Presents as a scrotal mass • Most tumors diagnosed early • No serologic tumor markers for seminoma • Treatment: surgery, radiation therapy & chemotherapy • Cure rate>90%
Gross features of seminoma: • Produces bulky masses, sometimes10x normal testis • Homogenous, grey-white, lobulated cut-surface, usually devoid of hemorrhage & necrosis • Replaces entire testis in half of cases
Histologic features of seminoma: • Composed of single cell type • Tumor cells have clear cytoplasm, filled with glycogen • Tumor cells are arranged in lobules which are surrounded by fibrous stroma • The fibrous septa are infiltrated by lymphocytes & plasma cells
Spermatocytic seminoma • Rare but distinct clinicopathologic variant of seminoma that occurs only in the descended testes of elderly men and forming about 5% of seminomas • The tumor is bilateral in about 6% of cases compared to about 2% in classic seminoma
Morphology of spermatocytic seminoma: • Gross:The tumor tends to be poorly demarcated, usually soft with a gelatinous or mucoid appearance. Cystic areas, especially in the center, are common but hemorrhage or necrosis is almost always absent. • Micro: Three populations of tumor cells, separated according to size, are seen: 1) small cells that superficially resemble lymphocytes, 2) intermediate or medium-sized cells, the commonest cell type, have round nuclei and finely granular chromatic pattern, and 3) large or giant cells.
Biological behaviour of spermatocytic seminoma: • Spermatocytic seminoma is an extremely indolent tumor with rather limited malignant potential and rarely if ever metastasizes.
Embryonal carcinoma • This subtype of GCTs represents the most primitive form of the NSGCTs. • It accounts for about 15 to 35% of testicular GCTs.
Grossly, the tumors are large, often hemorrhagic and necrotic producing a variegated cut surface.
Histologically, they are extremely pleomorphic and show a variety of patterns forming glands, tubules, and even primitive embryo-like structures. • Many mitotic figures are present.
Embryonal carcinoma: Sheets of cells with large, hyperchromatic nuclei, prominent nucleoli and poorly-defined cell borders
Embryonal carcinoma metastasizes early and widely via both lymphatic and hematogenous routes
Yolk Sac Tumor (Endodermal Sinus Tumor) • Testicular yolk sac tumors occur in two forms: either as a pure form in young children or as a focal differentiation within other NSGCTs, mainly embryonal carcinoma, in adults. • Pure YST of the adult testis is rare. • It is noted for its resemblance to rat fetal yolk sac and the presence of microscopically distinctive structures known as Schiller-Duval bodies.
Pathologic features of yolk sac tumor • Gross: The cut surface is gray-white and may be cystic.
Microscopic features of yolk sac tumor • Microscopically, the tumor shows a variety of patterns, the commonest of which is a loose meshwork of small spaces and cysts (producing a sieve-like appearance) lined by either flattened cells or vacuolated cells
Serum markers in yolk sac tumor (YST) • YST is almost invariably associated with production of large amounts of alpha-fetoprotein (AFP) and also alpha-1 antitrypsin (a -1AT). • AFP may be followed as a marker of disease progression in the patient's serum.
Teratoma • A tumor typically composed of several tissues representing two or more germinal layers • Teratomas are further subdivided into mature, immature and teratoma with malignant transformation
Mature teratoma showing cysts lined by mucous epithelium (left) and keratinizing squamous epithelium (right).
Immature teratoma with primitive brain tissue (upper left corner) and well-differentiated glands (lower half).
Choriocarcinoma • This is a highly malignant neoplasm that is usually widely disseminated and frequently fatal. • In this form of testicular GST the cells differentiate in the direction of trophoblastic (placental) tissue • The tumor typically presents in adolescent or young adults with widespread disease,
Microscopically, the tumor is composed of two types of cells: Syncytiotrophoblasts, large multinucleate cells with abundant vacuolated cytoplasm containing hCG and Cytotrophoblasts, polygonal cells with distinct cell borders and single nuclei, which grow in clusters and are surrounded by the syncytiotrophoblasts
Leydig cell tumor key facts: • Can develop at any age from infancy to old age • Most are benign, some are malignant • Most tumors are hormonally active, but some are inactive • May secrete androgens or estrogens -Androgen excess: Premature puberty & macrogenitosomia -Estrogen excess: Gynecomastia in adult males
Sertoli cell tumor • These tumors are more rare than Leydig cell tumors. • They elaborate androgens or estrogens. • Occasionally, they cause gynecomastia but sexual precocity is infrequent.
Important Qs • Investigation of male infertility • Classification of testicular tumors, both clinical as well as pathologic • Seminoma in detail • All germ cell tumors, in brief • Functional tumors of the testis • Serum markers for testicular tumors