Download
1 / 26
260 likes | 266 Views
Digital Health I. WEBS6202: Further Web Science. Catherine Pope 20 April 2015. What is Digital Health?.

E N D
Digital Health I WEBS6202: Further Web Science Catherine Pope 20 April 2015
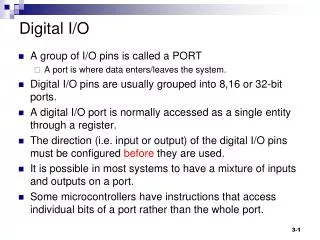
What is Digital Health? • hardware (monitors/sensors) software (algorithms) digitized health records and data linkage (esp genetics); Internet medicine; Heath information, big data; electronic communication; social networking • Health 2.0; Medicine 2.0 • eHealth, mHealth (mobile medicine) • Connected Health • Telecare/Telemedicine/Telehealth • “digitally engaged patient” “quantified self”
E-health - WHO definition (2012) the transfer of health resources and health care by electronic means. It encompasses three main areas: • The delivery of health information, for health professionals and health consumers, through the Internet and telecommunications. • Using the power of IT and e-commerce to improve public health services, e.g. through the education and training of health workers. • The use of e-commerce and e-business practices in health systems management. a new method for using health resources …in time should help to improve efficient use of these resources. The Internet also provides a new medium for information dissemination, and for interaction and collaboration among institutions, health professionals, health providers and the public.
an emerging field in the intersection of medical informatics, public health and business, referring to health services and information delivered or enhanced through the Internet and related technologies. In a broader sense, the term characterizes not only a technical development, but also a state-of-mind, a way of thinking, an attitude, and a commitment for networked, global thinking, to improve health care locally, regionally, and worldwide by using information and communication technology. Eysenbach G. (2001) J Med Internet Research 3(2)
Eysenbach’s 10 e’s. • Efficiency (avoid duplication, better communicaiton etc) • Enhanced quality of care • Evidence based medicine • Empower patients • Encourage shared decision making • Educate clinicians • Enable information transfer • Extend scope of care • Ethical challenges • Equity (access and benefit)
Reminder – the evolution of the relationship between the Web and medicine/health • Web 1.0: information transfer (tele-monitoring -medicine) • Web 2.0: interactivity • connect patients to providers (B2C model) • connect patients to each other (online support groups) • Web 3.0 • Semantic data linkage ?
Health and illness context • Demographic change developed world life expectancy from 40-80 in 200 years conditions associated with ageing e.g. arthritis, dementia long term conditions (chronic illness) & comorbidity • Increased cost of health services • Shift from repair to prevention and self care • Access (remote and rural populations and the less mobile)
UK Policy context – IT infrastructure • NHS Plan 2002 (modernisation) • Wanless Report 2002 (recommends doubling of spending on ICT to fund ambitious targets) • NPfIT 2002 (Connecting for health) • integrated care records service- electronic prescribing system- electronic appointment booking system- the IT infrastructure to support these systems. scrapped in Autumn 2011 • Wanless Report 2007 (ICT implementation = slow)
Medical Sociology does the internet Hardey, M (1999) Doctor in the House: the internet as a source of lay knowledge and the challenge to expertise SHI 21(6) 820-35 • Interview study 10 households 2 x per year the internet as information source • challenges medical expertise (empowers users/patients) • offers pluralistic approaches to health • will transform professional patient interactions
Digital health (digital sociology) • Critical digital health studies (Lupton, D. Sociology Compass 2014) – sociology, STS, media and cultural studies – critically address the socio-political and ethical dimensions of digital health • Digital sociology (Lupton, D. TASA conference paper 2013) – critical and reflexive • Theoretically informed - political economy; socio-technical; cyberculture • Substantive topics (websites; telemedicine; socio-economics (politics);digitised self) • Methodological challenges (digitised sociologists and ‘live’ dynamic approaches)
Plan • Next week – look in more detail at use of Web/internet and digitised self • Rest of today’s session review telemedicine/telehealth and begin the discussion about the ‘politics’ of. Readings and workshop this week - thinking about the big picture and look at techno-optimism Next week readings look at micro level, and then you have opportunity to think about the assessment & consolidate your learning on this topic.
Mair F, May C, Murray E et al (2009) Understanding the implementation and integration of E-Health Services http://www.sdo.nihr.ac.uk/projdetails.php?ref=08-1602-135 Methods: • Systematic review • Qualitative study of professionals (barriers and facilitators) • Case studies using qualitative and quantitative methods • Choose and Book • Picture Archiving • Clinical Nurse Information System – using PDAs
Definitional problems Telemedicine ? • what is eHealth? • Management systems (data storage and transfer); • communication systems (for users separated in space/time); • CDSS (rule based decision support); • Information resources - internet access to information. • Systematic reviews of implementation are misleading (methodological flaws and insufficient attention to the work required to bring systems into everyday use, or how eHealth systems impact on roles, responsibilities and tasks)
Choose and Book – variable implementation http://www.chooseandbook.nhs.uk/ • well integrated in hospital care: ‘We have got it in as mainstream business processes. My consultants are used to it ... it is becoming a way of life here…’ (CSI Chief Executive) • poor integration in GP: ‘And again for people to say that a Choose and Book takes two minutes – it just doesn’t – it is two minutes if you are really lucky, if the wind is in the right direction on the right day. Even if those 2 minutes but still 20% of the common consultation … 20% that wasn’t there before.’ (CS1 GP Early Adopter and IT enthusiast).
Picture archiving & communication system (PACS) http://www.connectingforhealth.nhs.uk/systemsandservices/pacs Fully normalized - highly integrated, enabled the organization to meet its goals more efficiently than the old system: ‘It [PACS] is firmly embedded. If you walk around this hospital two years on, the clinical team wouldn’t even stop to think about what’s they’re doing. It just, there’s not other way for them to get to look at the x-ray image. … No, no it’s truly embedded...’ (CS2 Hospital Chief Executive).
Barriers and facilitators 1. Patient benefits and clear purpose. 2. Collaborative working. 3. Standards a) universality, b) clinical risk, legality & safety. 4. Ease of use a) familiarity & ease to learn, b) efficiency and c) technical support. 5. Professional attitudes a) unity of purpose and b) sense of user empowerment & relationship with suppliers/designers. 6. Clear rationale. 7. Cost a) time, convenience & physical space and b) financial.
Mair et al conclusions • Need for three way dialogue between designers, implementers and professional users • Attend to • Context (national and local policy; championing and leadership) • Nature of the technology (usability; effects on interactions) • Impact on work, workload and training
Whole System Demonstrator cluster RCT Telehealth ? Telecare? • remote exchange of data between a patient and healthcare professionals (passive monitoring = telecare) • 6191 patients, 238 GP practices, 3 sites, Newham, Kent and Cornwall, 3 conditions diabetes, COPD and CHD Findings (my summary – go look it up!) Fewer deaths and emergency admissions (small decrease in admission to hospital, but NS impact on use of hospital services) Significant barriers to patient adoption (disruptive effects/ identity) Telehealth does not seem to be a cost effective addition to standard support and treatment
Whole system demonstrator programme: Headline findings – December 2011 “if delivered properly, telehealth can substantially reduce mortality, reduce the need for admissions to hospital, lower the number of bed days spent in hospital and reduce the time spent in A&E” https://www.gov.uk/government/news/whole-system-demonstrator-programme-headline-findings-december-2011
WSD References Steventon A et al. BMJ 2012; 344 doi: http://dx.doi.org/10.1136/bmj.e3874 Sanders C et al. BMC Health Services Research 2012, 12:220 doi:10.1186/1472-6963-12-220 Henderson C et al. BMJ 2013; 346 doi: http://dx.doi.org/10.1136/bmj.f1035
The politics of digital health • Power (digital literacy and socio-economic position) • Digital data (configuration, collation and use) • Neoliberalism (productive citizen and activated patients)
Digital Divide: Wyatt S, Thomas G, Teranova T. in Woolgar S (2002) Virtual Society Oxford: OUP • Resisters (don’t want to use) • Rejecters (stopped using) • Excluded (lack access) • Expelled (involuntarily lost access)
Who uses Web /internet (for health) • Income • Education • Age (mirrors existing social inequalities in health) See Oiihttp://www.oii.ox.ac.uk/ for more detailed descriptive data about digital literacy and access
Configuring data and users • Digital health information • Health professions and organisations • Commercial interests • Government • Patient (and public) networks Activity producing health related data and shaping users and technology (e.g. paitentslikeme)
Digital Data Study of PatientsLikeMe (Kallinikos & TempiniISR 2014) – observation of this social media platform – patients use of self-tracking tools, information searching and the data generated by their interactions with the platform • Mediation of apparently ‘free’ data entry by patients to inform medical research • Requires steady flow of data so enrol the patients via enabling features - constructed sociality • Generates specific expert work (for the patients and the organisation) which in turn shapes the data
Neoliberalism Andreasson H, Dyb K. Information, Communication & Society 2010;13 (7): 956–975 • New public management associated with individualising of healthcare – ‘responsibilisation’ and push to self care. Technology offered as a fix but used in unanticipated ways. Lupton D.Social Theory & Health 2012; 10: 229–244 • Surveillance and self monitoring – disruptive power effects (reconfigure health professionals and patients), but need to notice how the technologies reproduce inequalities