Download
1 / 35
510 likes | 926 Views
VAGINAL DISCHARGE. VAGINAL DISCHRGE. OBJECTIVES : 1.WHAT IS LEUCORRHOEA? 2.IS IT NORMAL? 3. NORMAL VS BNORMAL 4.CLASSIFICATION 5.COMMON CAUSES 6.CLINICAL FEATURES 7.EVALUATION 8.MANAGEMENT. LEUCORRHOEA. EXECESSIVE VAGINAL DISCHARGE NOT DUE TO INFECTION(EXECESSIVE

E N D
VAGINAL DISCHRGE OBJECTIVES : 1.WHAT IS LEUCORRHOEA? 2.IS IT NORMAL? 3. NORMAL VS BNORMAL 4.CLASSIFICATION 5.COMMON CAUSES 6.CLINICAL FEATURES 7.EVALUATION 8.MANAGEMENT
LEUCORRHOEA • EXECESSIVE VAGINAL DISCHARGE NOT DUE TO INFECTION(EXECESSIVE CERVICAL MUCUS OR VAGINAL TRANSUDATION) ECTROPION, CERVICAL TEARS.
IS VAGINAL DISCHARGE NORMAL? • COULD BE PATHOLOGICAL • YES –SOME SITUATIONS IT CAN BE - PUBERTAL - PREGNANCY - PREMENSTRUAL - OC PILLS -SCANTY,NO SMELL,WHITISH,NO ITCHING NOT BLOOD STAINED.
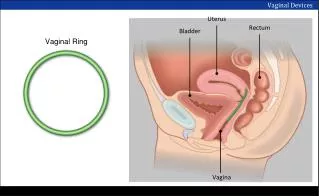
PHYSIOLOGY OF THE VAGINA • The vagina is lined by non-keratinized stratified squamous epithelial influenced by estrogen and progesterone • In children the pH of the vagina is 6-8 predominant flora is gram positive cocci and bacilli • At puberty, the vagina estrogenized and glycogen content increase.
Lactobacilli (Duoderline Bacilli) Convert glycogen to lactic acid pH of the vagina is 3.5-4.5
Vaginal Ecosystem • Dynamic equilibrium between microflora and metabollic by products of the microflora, host estrogen and vaginal pH • The predominant organism is aerobic
Factors affecting the vaginal Ecosystem • Antibiotics • Hormones or lack of hormones • Contraceptive preparations • Douches • Vaginal Medication • Sexual trauma • Stress • Diabetes Mellitus • Decrease host immunity – HIV + STEROIDS
Vaginal Desquamated Tissue • Reproductive age – superfacial cells (est) • Luteal phase- Intermediate cells (prog) • Postmenopausal women- parabasal cells ( absence of hormone)
CLASSIFICATION • PHYSIOLOGICAL • PATHIOLOGICAL - INFECTIVE - NON INFECTIVE- NEOPLASTIC - ATROPHIC - ALLERGIC,FB
INFECTIVE CAUSES • VAGINAL - CANDIDA VAGINITIS - TRICHOMONIAL VAGINITIS - BACTERIAL VAGINOSIS • CERVICAL - GONORRHOEA CERVICITIS - CHLAMYDIA CERVICITIS
CANDIDA VAGINITIS AGE- 20-40Y COMMON IN – PREGNANCY DIABETIC OBESE WOMEN FEATURES - CURDY WHITE,ITENSE ITCHING EXCORATION OF VULVA SMEAR- 10%KOH-FUNGAL HYPHE SEEN TREATMENT-CLOTRIMAZOLE-100MG BDx7D 200MGBDx3D RECURRENT -FLUCONOZLOE 150 MG WX4W
Symptoms: 20% asymptomatic • Pruritus • Vulvar burning • External dysuria • Dyspareunia • Vaginal discharge ( white, highly viscous, granular, has no odor)
Signs • Erythema • Oedema • Excoriation • Pustules • Speculum: cottage cheese type of discharge • Adherent thrush patches attached to the vaginal wall - pH is < 4.5
Investigation 1.Clinical 2. pH of the vagina norma < 4.5 3. Fungal element either budding yeast form or mycelia under the microscope 4. Whiff test is negative 5. Culture with Nickerson or Sabouraud media (Candida tropicalis)
Management • Standard • Topically applied azole ( nystatin) - 80% - 90% relief 3. Oral antifungal (Fluconazole) 4. Adjunctive treatment topical steroid - 1% hydrochortisone
TRICHOMONIAL VAGINITIS • AGENT - TRICHOMONIA VAGINALIS • AGE -20-40YRS,SEX ACTIVITY FEATURES GREENISH,FROTHY,COPIOUS,ITCHING STRAWBERRY SPOTS ON VAGINA VAG. SMEAR-MOTILE ORGANISMS TREATMENT- METRONIDAZOLE - 200XBDX7D OR400XBDX3 -COUPLE TREATED TOGETHER
BACTERIAL VAGINOSIS AGENT–G.VAGINALIS+ANAEROBIC AGE -20-40 YRS FEATURES-WHITISH GREY,COPIOUS NO ITCHING,FISHY SMELL VAG.SMEAR-CLUE CELLS TREATMENT-METRONIDAZOLE500XBD X7DAYS
SIGNS AND SYMPTOMS Symptoms: • 30-40% asymptomatic • Unpleasant vaginal odour (musty or fishy odor) • Vaginal discharge: thin, grayish, or white Signs: • Discharge is not adherent to the vagina, itching, burning is not usual
Diagnosis: • pH: 5-6.5 • Positive odor test- mix discharge with 10% KOH – fishy odor(metabollic by product of anaerobic amins the Whiff test) • Absence of irritation of the vagina and vulvar epithelium • Wet smear – clue cells -Vaginal epithelial cells with clusters of bacteria adherent to their external surface (2% - 5%). -Wet smear shows absent and lack of inflammatory cells.
Complication • Increase risk of pelvic inflammatory disease • Post operative cuff infection after hysterectomy • In pregnancy, it increase the risk of premature rupture of membrane • Premature labour, chorioamnionitis, endometritis
Management • Metronidazole 500 mg twice daily for 7 days Cure is 85% it fall to 50% if the partner is not treated • Clindamycine 300 mg twice daily • Vaginal
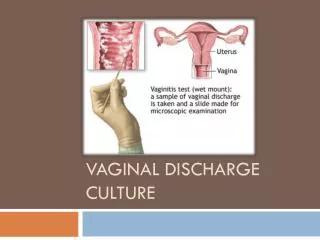
HOW TO ASSES..? DETAILED HISTORY COLOUR AMOUNT,SMELL,ITCHING RELATION TO COITUS /MENSES,pH CLINICAL EXAMINATION-EX GENITAL P/S EXAM INVESTIGATIONS-VAGINAL SMEAR -CULTURE
CERVICAL INFECTIONS GONORRHOEA-NEISS. GONORRHOEAE -85 %ASYMPTOMATIC - MUCOPURULANT - SMEAR FROM CX O&URETHRA - INTRACELL. GM –VE DIPLOCOCCI -SINGLE DOSE CEFETRIOXONE
CERVICAL INFECTIONS • CLAMYDIA-CL.TRACHOMATIS • AGE -20-40 • MUCOPURULANT • SEXUAL TRANSMITTED • FLOROSCENT ANTIBODY TEST/CULT. • DOXYCYCLINE 100XBDX7D