Download
1 / 16
260 likes | 2k Views
Vaginal Hysterectomy. Kaidy Waterman & Emily Beacham. Anatomy and Physiology. Removal of uterus Possible removal of fallopian tubes and ovaries Ligature of uterosacral ligaments Ligature of cardinal ligaments Ligature of uterine arteries

E N D
Vaginal Hysterectomy Kaidy Waterman & Emily Beacham
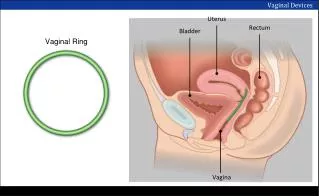
Anatomy and Physiology • Removal of uterus • Possible removal of fallopian tubes and ovaries • Ligature of uterosacral ligaments • Ligature of cardinal ligaments • Ligature of uterine arteries • Possible ligature of round ligament, ovarian ligament and fallopian tubes
Reasons for Procedure • Sterilization • Endometriosis • Fibroids • Cancer • Adhesions • Uterine prolapse • About 1/3 of all hysterectomies are done vaginally • Doctors prefer vaginal because it is less invasive • Laparoscopically assisted vaginal hysterectomies are becoming much more common
General Details Anesthesia and Positioning Skin Prep and Draping Vaginal prep Lithotomy drape • Anesthesia is general • Patient is in lithotomy position • Candy cane stirrups
Supplies, Equipment and Instruments • Auvard weighted speculum • Heaney/Deaverretracters • Tenaculum/Laheyvulsellum • #15 blade • #7 knife handle • 4X4 sponges • Peri-Pad • Heaney clamps • Mayo scissors • Long mayo • Kelly clamps • Schnidt • Pean • Jacob’s vulsellum • Foley catheter • Vag packing
Special Considerations • Careful with catheterization after the procedure • Care must be taken not to damage the fallopian tubes or ovaries if they are going to remain in the body
TIME OUT • Auvard weighted speculum is placed in the posterior vaginal wall • Heaney or Deavers retract the lateral vaginal walls • Tenaculum/Lahey placed at the edge of cervix to permit traction and movement. • D&C may be performed here
#15 blade on #7 handle, incise vaginal wall anteriorly around cervix • Blunt dissection, index and middle finger with 4X4, free bladder from anterior surface of the cervix • Deaver is placed anteriorly to elevate the bladder • Protects bladder • Visualization of peritoneum and anterior cul-de-sac
Use #15 knife blade, opening is made in the cul-de-sac • Peritoneum of posterior cul-de-sac is identified and incised with #15 • Uterosacral ligaments are doubly clamped with Heaney clamps, cut with Mayo and ligated. • Ligatures are not cut-left long and tagged with kelly
Manipulate uterus posteriorly, cardinal ligaments on each side are doubly clamped and cut with Mayos and ligated • Same is done with uterine arteries except the clamps are Kelly, Schnidt, or Pean • Fundus is put into the vaginal canal with previously placed tenaculum/Jacob’s vulsellum
If ovaries are preserved: • Round ligament • Ovarian ligament • Fallopian are doubly clamped with Heaney clamps, cut with mayo • Uterus is removed • Pedicles of the ligaments are ligated
Peritoneum between rectum and vagina is approximated with a continuous absorbable suture • Cul-de-sac is closed by placing sutures from vaginal wall through infundibulopelvic and round ligaments and back out through the vaginal wall, tied down on the vaginal portion of the vault • Round, uterosacral, and cardinal ligaments are individually approximated and reattached to the angle of the vagina • Foley catheter is placed, vagina is packed, perineal pad is placed.
Postoperative Care Complications Care and Prognosis Transport to PACU Return to normal activities • Bowel obstruction or damage • Bladder injury • Wound infection of dehiscence • Ureteral injuries • Hemorrhage
Pearl of Wisdom Some surgeons complete actions on one side of the uterus then move to the other side; some alternate sides as they move caudally. The STSR must adjust to the pattern and be sure to have an adequate supply of homeostasis.