Download
1 / 74
1.31k likes | 2.91k Views
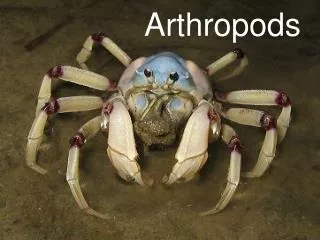
ARTHROPODS OF MEDICAL IMPORTANCE. Arthropods (2 hours). 1. Defines “Arthropod’’ 1.1 Lists the arthropod classification. 2. Lists the clinical tables related with arthropods 2.1. Defines the cklinical importance of arthropodsi . 2.2. Lists the prevention methods from arthropods.

E N D
Arthropods (2 hours) • 1. Defines “Arthropod’’ • 1.1 Lists the arthropod classification. • 2. Lists the clinical tables related with arthropods • 2.1. Defines the cklinical importance of arthropodsi. • 2.2. Lists the prevention methods from arthropods. • 2.3. Lists the laboratory diagnostic methods.
ARTHROPODA • Arachnidia • Diplopoda • Chilopoda • Insecta • Crustacea
Myriapoda/Centipedes • The centipedes are elongated, multisegmented (15 to more than 181 segments), many-legged, tracheate arthropods. • They possess a distinct head and trunk. • The body is dorsoventrally flattened, and each trunk segment bears a single pair of legs. • Maxillipeds or poison claws are situated on the first segment and are used for capturing prey.
commonly found in dark, damp environments such as the areas beneath logs, among rubbish, and inside old buildings. • Human bites are almost invariably the result of accidental exposure to the organism during outdoor activities. • Centipede bites may be extremely painful and cause swelling at the site of the bite.
Pentastomida/Tongue Worms • The pentastomids, or tongue worms, are bloodsucking endoparasites of reptiles, birds, and mammals. • Many vertebrates, including humans, may serve as intermediate hosts. • contaminate vegetation or water, which is in turn ingested by one of several possible intermediate hosts (fish, rodents, goats, sheep, or humans).
Humans may also become infected by ingesting the inadequately cooked flesh of infected reptiles or other definitive hosts or by eating the infected flesh of intermediate hosts (e.g., goats, sheep) containing infective larvae. • In this case, the human host is considered a temporary definitive host.
the infection is acquired by ingesting raw vegetables or water contaminated with pentastome eggs or by consuming raw or undercooked flesh of infected animals. • Treatment is not usually warranted.
Crustacea/Copepods,Decapods • The crustaceans are primarily gill-breathing arthropods of fresh and salt water. • found in fresh water and serve as intermediate hosts of various worms Copepods • small, simple aquatic organisms. They lack a carapace, have one pair of maxillae, and have five pairs of biramous swimming legs. Free and parasitic forms exist. The genera Diaptomus and Cyclops are medically important.
intermediate host in the life cycle of several human parasites, including Dracunculus medinensis (dracunculiasis), Diphyllobothrium latum (diphyllobothriasis), • Copepods have a worldwide distribution • the chlorination and filtration of water and thorough cooking of all fish. • Infected people must not be allowed to bathe in water used for drinking, and suspected water should be avoided.
Decapods • include the prawns, shrimps, lobsters, crayfish, and crabs. • Crabs and crayfish are medically important as the second intermediate hosts of the lung flukeP. westermani. • Thorough cooking of crabs and crayfish is the most effective means of preventing infection with P. westermani.
Chelicerata (Arachnida) • Spiders • characteristic features that permit easy identification. Specifically, they possess eight legs, no antennae, a body divided into two regions (cephalothorax and abdomen), and an unsegmented abdomen with spinnerets posteriorly. All true spiders produce venom and kill their prey by biting • Venomous spiders may be classified as those that cause systemic arachnidism and those that cause necrotic arachnidism. • Systemic arachnidism is primarily caused by tarantulas and black widow spiders. • Tarantulas (family Theraphosidae) are large, hairy spiders of the tropics and subtropics. The tarantulas are of little importance because they are not very aggressive and avoid human habitations.
The black widow spider, Latrodectus mactans, is widespread through the southern and western United States. • Related species of Latrodectus are found throughout temperate and tropical regions of all continents, but none is primarily domestic; thus their contact with humans is limited. Black Widow Spiders • The female black widow spider (L. mactans) is easily recognized by the presence of a globose, shiny, black abdomen bearing the characteristic orange or reddish hourglass marking on the ventral surface. The venom of the black widow spider is a potent peripheral neurotoxin • Only the female Latrodectus spider is dangerous to humans; the small, feeble male delivers an ineffective bite.
These spiders frequent wood and brush piles, old wooden buildings, cellars, hollow logs, and privies. • Given these locations, the bite is often located on the genitalia, buttocks, or extremities. • Healthy adults usually recover, but small children or weakened people suffer considerably from these bites and may die without treatment.
Muscle spasms may be severe and may require the intravenous administration of calcium gluconate or other muscle relaxant agents. • A specific antivenin is available and remains the treatment of choice. It is valuable if given shortly after the bite.
Brown Recluse Spiders • Spiders producing necrotic arachnidism belong to the genus Loxosceles. These spiders are yellow to brown and are of medium size (5 to 10 mm long) with relatively long legs. They commonly display two distinguishing characteristics: a dark fiddle- or violin-shaped marking on the dorsal side of the cephalothorax, and six eyes arranged in three pairs forming a semicircle. • The venom injected by the female or male spider is a necrotoxin (that may also have hemolytic properties) and causes necrotic lesions with deep tissue damage. Humans are bitten only when the spider is threatened or disturbed.
Initially, the bite of Loxosceles species tends to be painless; however, several hours later, itching, swelling, and soreness may develop in the area of the bite. • Intravascular coagulation and hemolysis may occur and be accompanied by hemoglobinuria and cardiac and renal failure. This hemolytic syndrome may be life threatening and occurs more commonly after the bite of L. laeta. In South America, this syndrome is known as visceral loxoscelism.
Cleansing the bite wound and providing tetanus prophylaxis and antibiotics to prevent secondary infection may all be indicated. • Healing is generally uncomplicated, and debridement or excision should not be performed for 3 to 6 weeks to allow natural healing to commence.
Excision and skin grafting may be necessary for bites that have not healed in 6 to 8 weeks. • Systemic therapy with corticosteroids may be useful in treating the hemolytic syndrome • Preventive measures are similar to those recommended for black widow spiders. Loxosceles (and other) spiders may be controlled in dwellings with insecticide compounds.
Scorpions • The typical scorpion is elongated with conspicuous, pincher-like claws (or pedipalps) at the anterior end of the body, four pairs of walking legs, and a distinctly regimented abdomen that tapers to a curved, hollow, needle-like stinger. • When the scorpion is disturbed, it uses the stinger for defense. Both male and female scorpions can sting. Venom is injected through the stinger from two venom glands in the abdomen. Most scorpions are unable to penetrate human skin or inject enough venom to cause real damage; however, a few species are capable of inflicting painful wounds that may cause death.
Children under the age of 5 years are most likely to be fatally stung by scorpions. • Scorpions are nocturnal, and during the day they remain concealed under logs, rocks, and other dark, moist places. They invade human habitations at night, where they may hide in shoes, towels, clothing, and closets.
The effect of a scorpion sting in a patient is highly variable and depends on factors such as the species and age of the scorpion, the kind and amount of venom injected, and the age, size, and sensitivity of the person who was stung. • Although the sting of many scorpions is relatively nontoxic and produces only local symptoms, other stings may be quite serious. • Scorpions produce two types of venom: a neurotoxin and a hemorrhagic or hemolytic toxin. The hemolytic toxin is responsible for local reactions at the site of the sting, including radiating, burning pain; swelling; discoloration; and necrosis. The neurotoxin produces minimal local reaction but rather severe systemic effects, including chills, diaphoresis, excessive salivation, difficulty speaking and swallowing, muscle spasm, tachycardia, and generalized seizures. In severe cases, death may result from pulmonary edema and respiratory paralysis.
Local or systemic signs and symptoms coupled with physical evidence of a single point of skin penetration are usually sufficient to establish the diagnosis. • An entomologist or parasitologist should be consulted if there is a taxonomic question.
The management of scorpion stings varies. In the absence of systemic symptoms, palliative treatment may be all that is necessary. Pain may be relieved by analgesics or local injection of Xylocaine; however, opiates appear to increase toxicity. • Local cryotherapy may reduce swelling and retard the systemic absorption of the toxin. Hot packs produce vasodilatation and may accelerate toxin distribution systemically and are therefore contraindicated.
Antivenin is available and is effective if administered soon after the sting. Very young children with systemic symptoms should be treated as medical emergencies. Systemic symptoms and shock should be treated supportively. • The use of chemical pesticides to reduce scorpion populations. Removal of debris around dwellings can reduce hiding and breeding places.
Mites • small, eight-legged arthropods characterized by a saclike body and no antennae. A large number of mite species are free-living or are normally associated with other vertebrates (e.g., birds, rodents) and may cause dermatitis in humans on rare occasions. • The number of mites that are considered true human parasites or present real medical problems is quite small and include the human itch mite (Sarcoptes scabiei), the human follicle mite (Demodex folliculorum), and the chigger mite. • Mites affect humans in three ways: by causing dermatitis, by serving as vectors of infectious diseases, and by acting as a source of allergens.
The itch mite (S. scabiei) • causes an infectious skin disease variably known as scabies, mange, or the itch. The adult mites average 300 to 400 μm in length with an oval, saclike body in which the first and second pairs of legs are widely separated from the third and fourth pairs. The body has dorsal transverse parallel ridges, spines, and hairs. The ova measure 100 to 150 μm. • Adult mites enter the skin, creating serpiginous burrows in the upper layers of the epidermis. The female mite lays her eggs in the skin burrows, and the larval and nymph stages that develop also burrow in the skin. The female mites live and deposit eggs and feces in epidermal burrows for up to 2 months. Characteristically, the preferred sites of infestation are the interdigital and popliteal folds, the wrist and inguinal regions, and the inframammary folds. The presence of the mites and their secretions cause intense itching of the involved areas. The mite is an obligate parasite and can perpetuate itself in a single host indefinitely.
Scabies • is cosmopolitan in distribution, with an estimated global prevalence of about 300 million cases. The mite is an obligate parasite of domestic animals and humans; however, it may survive for hours to days away from the host, thus facilitating its spread. • Transmission is accomplished by direct contact or by contact with contaminated objects such as clothing. • Sexual transmission has been well documented. Spread of the infection to other areas of the body is accomplished by scratching and manual transfer of the mite by the affected person. • Scabies may occur in epidemic fashion among people in crowded conditions such as daycare centers, nursing homes, military camps, and prisons.
The outstanding clinical diagnostic symptom is intense itching, usually in the interdigital folds and sides of the fingers, buttocks, external genitalia, wrists, and elbows. The uncomplicated lesions appear as short, slightly raised cutaneous burrows. • At the end of the burrow, there is frequently a vesicle containing the female mite. The intense pruritus usually leads to excoriation of the skin secondary to scratching, which in turn produces crusts and secondary bacterial infection. • Patients experience their first symptoms within weeks to months after exposure; however, the incubation period may be as little as 1 to 4 days in persons sensitized by prior exposure. • Host hypersensitivity (delayed or type IV) probably plays an important role in determining the variable clinical manifestations of scabies.
Some immunodeficient people may develop a variant of scabies, so-called Norwegian scabies, characterized by generalized dermatitis with extensive scaling and crusting and the presence of thousands of mites in the epidermis. This disease is highly contagious and suggests that host immunity also plays a role in suppressing S. scabiei. • The clinical diagnosis of scabies is based on the characteristic lesions and their distribution. The definitive diagnosis of scabies depends on the demonstration of the mite in skin scrapings. Because the adult mite is most frequently found in the terminal portions of a fresh burrow, it is best to make scrapings in these areas. • The scrapings are placed on a clean microscope slide, cleared by the addition of 1 or 2 drops of a 20% solution of potassium hydroxide, covered with a coverslip, and examined under a low-power microscope. With experience, the mite and ova may be recognized. Skin biopsy may also reveal the mites and ova in tissue sections.
The standard, and very effective, treatment for scabies is 1% gamma benzene hexachloride (lindane) in a lotion base. One or two applications (head to toe) at weekly intervals is effective against scabies. Lindane is absorbed through the skin, and repeated applications may be toxic. For this reason, it is not advisable to use it in treating infants, small children, or pregnant or lactating women. • Recently, a 5% permethrin cream (Elimite) has replaced lindane lotions as the treatment of choice for scabies. Clinical trials have shown permethrin to be more effective and less toxic than lindane. • Other preparations used to treat scabies include crotamiton sulfur (6%) preparations, benzyl benzoate, and tetraethylthiuram monosulfide.
Primary prevention of scabies is best achieved with good hygiene habits, personal cleanliness, and routine washing of clothing and bed linens. • Secondary prevention includes the identification and treatment of infected people and possibly their household and sexual contacts. In an epidemic situation, simultaneous treatment of all affected people and their contacts may be necessary. This is followed by thorough cleansing of the environment (e.g., boiling clothing and linens) and ongoing surveillance to prevent re-occurrence.
Human Follicle Mites • include two species of the genus Demodex, D. folliculorum and D. brevis. These mites are minute (0.1 to 0.4 mm) organisms with a wormlike body, four pairs of stubby legs, and an annulate abdomen. • D. folliculorum parasitizes the hair follicles of the face of most adult humans, whereas D. brevis is found in the sebaceous glands of the head and trunk. Infestations are uncommon in young children and increase at the time of puberty. It is estimated that 50% to 100% of adults are infested with these mites. • The role of Demodex species in human disease is uncertain. They have been associated with acne, blackheads, blepharitis, abnormalities of the scalp, and truncal rashes. More recently, extensive papular folliculitis resulting from Demodex infestation has been described in people with acquired immunodeficiency.
Factors such as poor personal hygiene, increased sebum production, mite hypersensitivity, and immunosuppression may increase host susceptibility and enhance the clinical presentation of Demodex infestation. Most people infested with these mites remain asymptomatic. • Mites may be demonstrated microscopically in material expressed from an infested follicle. They may be seen as incidental findings in histologic sections of facial skin. • Effective treatment consists of a single application of 1% gamma benzene hexachloride.
Chigger Mites • the larvae of mites of the family Trombiculidae. The adult trombiculid mites infest grass and bushes, and their larvae (i.e., chiggers) attack humans and other vertebrates, producing severe dermatitis. The larvae have three pairs of legs and are covered with characteristic branched, featherlike hairs. • The larvae appear as minute, barely visible, reddish dots attached to the skin, where they use their hooked mouth parts to ingest tissue fluids. Chiggers typically attach to the skin areas where clothing is tight or restricted such as the wrists, ankles, armpits, groin, and waistline. • Chiggers are a particular problem for outdoor enthusiasts such as campers and picnickers. In Europe and the Americas, they are associated with intensely pruritic lesions; however, in Asia, Australia, and the western Pacific rim, they serve as vectors of the rickettsial disease scrub typhus or tsutsugamushi fever (Rickettsia tsutsugamushi)
Saliva injected into the skin at the time of mite attachment produces an intense pruritus and dermatitis. The skin lesions appear as small erythematous marks that progress to papules and may persist for weeks. Mite larvae may be visible in the center of the reddened, swollen area. The irritation may be so severe that it causes fever and sleep disruption. Secondary bacterial infection of the excoriated lesions may occur. • Treatment for dermatitis caused by chiggers is largely symptomatic and consists of antipruritics, antihistamines, and steroids. The use of insect repellents such as N,N-9-diethyl-m-toluamide (DEET) may be of some help in prevention for persons going into chigger-infested areas
Ticks • bloodsucking ectoparasites of a number of vertebrates, including humans. • opportunistic rather than host specific and tend to suck blood from a number of large and small animals. • four-stage life cycle that includes the egg, larva, nymph, and adult. Although the larva, nymph, and adults are all bloodsuckers, it is the adult tick that usually bites humans. • comprise two large families, the Ixodidae, or hard ticks, and the Argasidae, or soft ticks.
Soft ticks have a leathery body that lacks a hard dorsal scutum, and the mouthparts are located ventrally and are not visible from above. • Hard ticks have a hard dorsal plate or scutum, and the mouthparts are clearly visible from above. • Soft ticks differ from hard ticks primarily in their feeding behavior. • Soft ticks complete engorgement in a matter of minutes or at most a few hours; hard ticks feed slowly, taking 7 to 9 days to become engorged.
Hard tick • Rocky Mountain spotted fever (Dermacentor species), tularemia (Dermacentor species), Q fever (Dermacentor species), Lyme disease (Ixodes species), babesiosis (Ixodes species), and ehrlichiosis (D. variabilis and A. americanum) Soft ticks • of the genus Ornithodoros transmit relapsing fever spirochetes (Borrelia species) in limited areas in the West. In general, people at risk for tick exposure are involved in outdoor activities in wooded areas. Tick exposure may also occur during stays in rural cabins inhabited by small rodents, which commonly serve as hosts for ticks and other ectoparasites. • Tick bites are generally of minor consequence and are limited to small erythematous papules. More serious consequences of tick bite include the development of a type of paralysis resulting from substances released by ticks during feeding and transmission of a number of rickettsial, bacterial, viral, spirochetal, and protozoan diseases of humans and other animals.
Ticks may attach at any point on the body but typically favor the scalp, hairline, ears, axillae, and groin. The initial bite is usually painless, and the presence of the tick may not be detected for several hours after contact. • After the tick has dropped off or has been removed manually, the area may become reddened, painful, and pruritic. The wound may become secondarily infected and necrotic, particularly if the mouthparts remain attached after manual removal
Three species of tick, D. andersoni, D. variabilis, and A. americanum, have all been reported to cause tick paralysis. This is characterized by an ascending flaccid paralysis, fever, and general intoxication, which may lead to respiratory compromise and death. The paralysis is due to toxic substances released in the saliva of the tick and may be reversed by tick removal. Tick paralysis is observed more commonly in young children and when tick attachment is in opposition to the central nervous system (e.g., scalp, head, neck). • Ticks are also involved in the transmission of infections such as Lyme disease, Rocky Mountain spotted fever, ehrlichiosis, Colorado tick fever, relapsing fever, tularemia, Q fever, and babesiosis. The identification of an organism as an adult tick is usually straightforward and based on the observations of an organism that is dorsoventrally flattened and possesses four pairs of legs and no visible segmentation
An entomologist or parasitologist should be consulted if further identification is desired. • Treatment, Prevention, and Control • Early removal of attached ticks is of primary importance and may be accomplished by steady traction on the tick body, grasped with forceps as close to the skin as possible. • Care should be taken to avoid twisting or crushing the tick, which may leave the mouthparts attached to the skin or inject potentially infectious material into the wound. • Because ticks may harbor highly infectious agents, the clinician should use appropriate infection-control precautions (e.g., use of gloves, handwashing, proper disposal of ticks and contaminated material) during tick removal. • Preventive measures used in tick-infested areas include the wearing of protective clothing that fits snugly about the ankles, wrists, waist, and neck so that ticks cannot gain access to the skin. Insect repellents such as N,N-9-diethyl-m-toluamide (DEET) are generally effective. People and pets should be inspected for ticks after visits to tick-infested areas.
Insecta • The insects, or hexapods, constitute the largest and most important of all the classes of arthropods, accounting for approximately 70% of all known species of animals. Insects include animals such as mosquitoes, flies, fleas, lice, roaches, bees, wasps, beetles, and moths to name just a few. • The insect body is divided into three parts-head, thorax, and abdomen-and is equipped with one pair of antennae, three pairs of appendages, and one or two pairs of wings or no wings at all. The medical significance of any insect is related to its way of life, particularly its mouthparts and feeding habits. • Insects may serve as vectors for a number of bacterial, viral, protozoan, and metazoan pathogens. Certain insects may serve merely as mechanical vectors for the transmission of pathogens, whereas in other insects the pathogens undergo multiplication or cyclic development within the insect host. • Insects can also be pathogens themselves by causing mechanical injury through bites, chemical injury through the injection of toxins, and allergic reactions to materials transmitted by bites or stings.
Bloodsucking Diptera • All dipterans have a single pair of functional membranous wings and various modifications of the mouthparts, which have been adapted for piercing the skin and sucking blood or tissue juices. Their most important feature is their role as mechanical or biologic vectors of a number of infectious diseases, including leishmaniasis, trypanosomiasis, malaria, filariasis, onchocerciasis, tularemia, bartonellosis, and the viral encephalitides. • The bloodsucking flies include mosquitoes, sand flies, and blackflies, all of which are capable of transmitting diseases to humans. Other dipterans, such as horse flies and stable flies, are capable of inflicting painful bites but are not known to transmit human pathogens. • Although the common housefly does not bite, it certainly is capable of mechanical transmission of a number of viral, bacterial, and protozoan infections to human hosts.
Mosquitoes • Adult mosquitoes are small and have delicate legs, one pair of wings, long antennae, and greatly elongated mouthparts adapted for piercing and sucking. The two major families of mosquitoes (Culicidae), the Anophelinae and the Culicinae, share a number of similarities in their life cycles and development. • They lay eggs on or near water, are good fliers, and feed on nectar and sugars. The females of most species also feed on blood, which they require for each clutch of 100 to 200 eggs. Females may take a blood meal every 2 to 4 days. In the act of feeding, the female mosquito injects saliva, which produces mechanical damage to the host but also may transmit disease and produce immediate and delayed immune reactions. • the genus Anopheles contains the species responsible for the transmission of human malaria. In the tropics, these mosquitoes breed continually in relation to rainfall. A. aegypti, the yellow fever mosquito, usually breeds in man-made containers (flower pots, gutters, cans) and is the primary vector of yellow fever and dengue in urban environments throughout the world. Body_ID:
The bite is usually followed within a few minutes by a small, flat weal surrounded by a red flare. The delayed reaction consists of itching, swelling, and reddening of the wound region. Secondary infection may follow as a result of scratching. • Medical attention is usually not sought for a bite unless secondary infection occurs. Local anesthetics or antihistamines may be useful in treating reactions to mosquito bites. • Preventive measures in mosquito-infested areas include the use of window screens, netting, and protective clothing. Insect repellents such as DEET are generally effective. Mosquito-control measures that involve the use of insecticides have been effective in some areas.