Download
1 / 15
150 likes | 168 Views
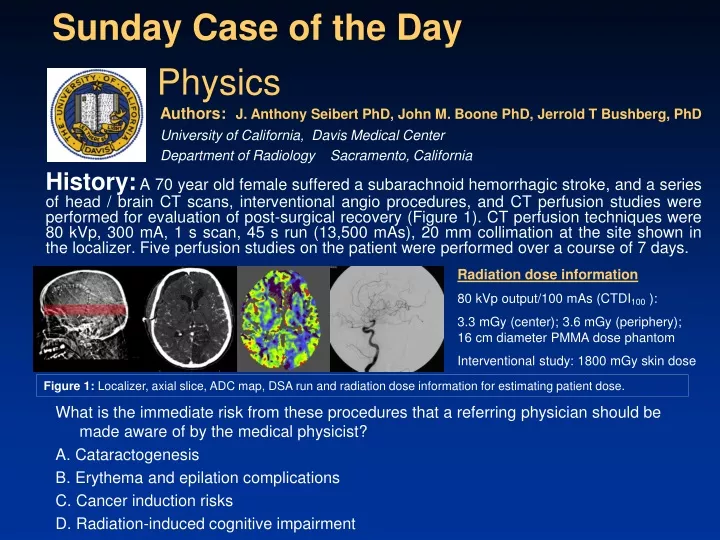
Sunday Case of the Day. What is the immediate risk from these procedures that a referring physician should be made aware of by the medical physicist? A. Cataractogenesis B. Erythema and epilation complications C. Cancer induction risks D. Radiation-induced cognitive impairment.

E N D
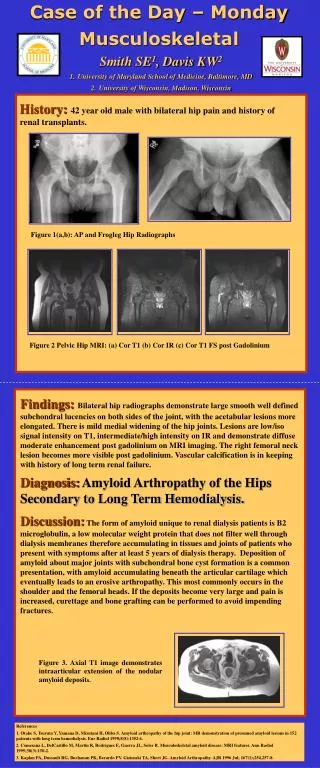
Sunday Case of the Day What is the immediate risk from these procedures that a referring physician should be made aware of by the medical physicist? A. Cataractogenesis B. Erythema and epilation complications C. Cancer induction risks D. Radiation-induced cognitive impairment History:A 70 year old female suffered a subarachnoid hemorrhagic stroke, and a series of head / brain CT scans, interventional angio procedures, and CT perfusion studies were performed for evaluation of post-surgical recovery (Figure 1). CT perfusion techniques were 80 kVp, 300 mA, 1 s scan, 45 s run (13,500 mAs), 20 mm collimation at the site shown in the localizer. Five perfusion studies on the patient were performed over a course of 7 days. Physics Authors: J. Anthony Seibert PhD, John M. Boone PhD, Jerrold T Bushberg, PhD University of California, Davis Medical Center Department of Radiology Sacramento, California Radiation dose information 80 kVp output/100 mAs (CTDI100 ): 3.3 mGy (center); 3.6 mGy (periphery); 16 cm diameter PMMA dose phantom Interventional study: 1800 mGy skin dose Figure 1: Localizer, axial slice, ADC map, DSA run and radiation dose information for estimating patient dose.
Findings:Upon follow-up about 2 weeks after the imaging exams were completed, this patient presented with erythema and epilation in the area of the CT perfusion scan, indicating a likely acute radiation dose of 3 Gy or more to the skin areas irradiated during the exam, which would include radiation dose from the interventional angiogram study as well as any other CT exams.
Diagnosis:B.In situations such as CT perfusion, which uses no table motion but involves many CT scans performed over time (e.g., in this case, 45 × 5 = 225 scans over a week long period), dose to a small volume of the patient can be quite high. This results in a large peak dose within the volume irradiated with special concerns at the skin surface. Deterministic acute effects of erythema (skin reddening) and epilation (hair loss) at the areas of the CT scan (plus accumulated radiation dose from other contemporaneous studies) are indicative of high skin dose in the range of 2 Gy for onset of erythema to 3 Gy and above for temporary epilation.
Radiation Induced Skin EffectsTransient & Main Erythema • Transient Erythema • Due to release of vasoactive amines (capillary vasodilatation / leakage / edema) • May appears within hours (the higher the dose the more rapid the onset) • Increases during the first week and often fades during the second week (dose dependent) • Threshold Acute Dose of >~5-6 Gy for small skin areas or >~2Gy for large fields or whole body exposure • Main Erythema • Threshold Acute Dose of >~6 Gy • Due to blood vessel damage (obstructive changes to arterioles) • Appears 2-3 weeks after exposure • Last for 3-4 weeks • Blue/mauve skin discoloration • Skin is warm, edematous, tender (often exhibits a burning sensation) F-18 FDG Contamination From : IAEA Information For Health Professionals, Reference 1. Fluoroscopy: 4 coronary artery stents with complications lasted 4.5 hours: appearance @ 7wks From :FA Henry et al., Reference 2.
Some Variables with Radiation Induced Skin Effects • Dose & Dose Rate ( For all endpoints, the higher the dose and dose rate (beyond the threshold for effects) the shorter the latency and more severe the effect • Fractionation (e.g., Main Erythema: Single Dose ~ 6 Gy vs. 3 doses in 3 days ~9 Gy) • Size of exposure area (e.g., Dose required for dermal necrosis @ 1 cm2 ~4.5 Gy vs. @ 10 cm2 ~2.2 Gy) • Anatomical location (e.g., Sensitivity to radiation induced erosive effects: Axilla > Face > Scalp > Palms)
Some Variables with Radiation Induced Skin Effects • Age at exposure (Children are more sensitive but often recover more quickly) • State of health (e.g., anemia and poor vascularization decrease the intensity of the erythema response while patients with hypothryoidism are more radiosensitive than euthyroid [normal thyroid function] individuals) • Combination of effects (e.g., Sensitivity to epilation is partly due to cell kinetics—thus slow growing can be a function of age and anatomical location
Radiation Induced Skin Injuries and Latent Period Effect Dose (Gy) Latent Period Early Transient Erythema ~3 hours Temporary Epilation ~3 3-4 wks Main Erythema ~6 2-3 wks Permanent Epilation ~7 1-3 wks Dry Desquamation ~12 4 wks Moist Desquamation ~15-20 3-4 wks Ulceration ~20 >2 wks Dermal Necrosis > 25 >3 wks
Discussion: • Typical dose information provided by most modern CT scanners includes the computed tomography dose index CTDIvol (mGy) and dose length product DLP (mGy-cm). These values are derived from measurements on specific CT scanners made with cylindrical plastic phantoms of two diameters (16 cm and 32 cm) to measure the CTDI100 with a 100 mm pencil chamber in a center and peripheral position3. • Weighted CTDI, CTDIw (mGy) = 1/3 center CTDI100 + 2/3 peripheral CTDI100 • Volume CTDI, CTDIvol (mGy) = CTDIw / pitch • DLP (mGy-cm) = CTDIvol × scan length (cm) • Effective dose (mSv) = DLP (mGy-cm) ×k (mSv / mGy-cm) • where k is dependent on scanned region constant derived from measurements and simulations as described in reference 3. • So how does the physicist calculate relevant dose metrics for this case, given the information provided with the history? Three explanations follow: • Peak skin dose is important for explaining the deterministic effects. The • CT dose estimate for the skin is approximated by CTDI100 peripheral, as: • 3.6 mGy/100 mAs × 13,500 mAs/study × 5 studies = 2430 mGy = 2.43 Gy
Discussion (cont): Adding the dose from the interventional study of 1.8 Gy results in a total estimated peak skin dose of 4.2 Gy. However, using the peripheral CTDI100 as a point dose measurement is flawed, as pointed out by Bauhs, et.al.4 The CTDI100 is a method used for situations where the table is incremented in conjunction with tube rotation to estimate multiple scan average dose, and will lead to an overestimate by nearly a factor of 2 (202 / 392) as shown in Figure 4 (reproduced from reference 4 as Table 3, below). Thus, a more realistic estimate of the peak skin dose is 2.43 Gy / 2 + 1.8 Gy 3.0 Gy Figure 4: Table 3 from Bauhs, et al.4 indicating point dose and CTDI100 measurements (highlighted) for perfusion study.
Discussion (cont): (2) Calculation of effective dose is determined from the DLP and the normalized effective dose per dose length product constant, k, obtained in Figure 5 below. CTDIvol /study (pitch=1) is calculated from CTDI100 central & peripheral values as: (1/3 (3.3 mGy/100 mAs)+2/3(3.6 mGy/100 mAs))×13,500 mAs = 473 mGy DLP is calculated from the CTDIvol (20 mm collimation) and the k value as: DLP = 473 mGy × 2 cm × 0.0021 mSv/mGy-cm 2 mSv / study The effective dose estimate for the 5 CT studies is thus 10 mSv. In order to determine the overall effective dose, the interventional angio effective dose (calculations not described) and other effective doses would be added. Figure 5: Table 3 reproduced from reference 4, indicating the k value for the adult head of 0.0021 mSv mGy-1 cm-1.
Discussion (cont): (3) An alternative dose tool is available with the ImPACT CT Patient Dosimetry Calculator5, which uses a methodology to calculate individual organ doses and effective dose by having relevant CTDI measurements (selectable for most modern CT scanners) and an anthropomorphic (adult) phantom to identify areas scanned. Figure 6 shows an example for one CT perfusion study this patient. Figure 6: The output data from the CT dosimetry tool5. On the left is the spreadsheet with parameters and data output; on the right is the scan positioning location details for this particular study.
Discussion (cont): Of note is the calculated effective dose of 3.2 mSv for the single perfusion study by ImPACT, higher than the calculation performed from the raw data of 2 mSv. This is possibly due to the use of a single slab of irradiated tissue for the estimate that uses a scanned area of the head/brain. The variation of the k factor determined from whole head scans could also result in the discrepancy. The effective dose estimation is a method to average a partial irradiation over the total body. For CT procedures such as brain perfusion studies where a small volume is irradiated to a high peak dose, the effective dose, while potentially a good indicator of stochastic risks such as cancer induction, is not particularly “effective” in indicating potential deterministic effects such as erythema. When effective dose is used as a surrogate for deterministic effects and peak doses, the “low” effective dose values in these situations where the volume is small and repeatedly scanned can cause overconfidence in the relative presumed safety of CT exams, certainly not warranted as shown in this case. With the above discussion, explanations for the other distracters in the original question are explained on the following slide.
What is the immediate risk from these procedures that a referring physician should be made aware of by the medical physicist? A. Cataractogenesis B. Erythema and epilation complications C. Cancer induction risks D. Radiation-induced cognitive impairment Discussion (cont): A. Cataractogenesis: While radiation-induced cataracts are certainly a concern for deterministic effects, particularly for doses of 1 Gy and above, the development of cataracts takes years, and for a 70 year old patient who has had a stroke, this is of secondary importance and lower risk relative to the erythema and epilation issues. C. Cancer induction risks: Development of radiation-induced cancer is certainly a long-term concern, particularly for the younger patient population who are more radiosensitive and have a much greater likelihood of expressing the cancer over their lifetime. While the effective dose is an indicator of this risk, still unknown are the potentially deleterious effects resulting from extremely high doses to particularly sensitive organs, and whether averaging over the total body is the correct approach. D. Radiation-induced cognitive impairment: The brain tissues are relatively radiation insensitive, and would take a significant whole brain exposure to demonstrate such an outcome. For this patient with a stroke, cognitive impairment has occurred by other damage independent of the radiation exposure.
Summary: The use of CT is increasing, as are many “non-invasive” CT examinations that can result in radiation-induced deterministic effects as well as stochastic effects. Medical care-givers that use CT and other diagnostic imaging devices for diagnostic and interventional procedures must become cognizant of the ionizing radiation risks, the methods for estimating dose, and the potential pitfalls of incomplete understanding of “radiation dose”. Use of CTDI is problematic, but it is the currently accepted method of estimating patient dose. Knowledge of the drawbacks can be taken into account to increase estimation accuracy. This physics case of the day demonstrates that radiation dose estimates for CT dosimetry can be described in several different ways. In particular, peak dose estimates for deterministic effects and effective dose for stochastic effects are very important. Medical physicists, radiologists, and CT technologists must become conversant and understanding of these radiation dose issues and the dose metrics available on modern CT scanners so that potentially dangerous radiation safety issues can be identified and corrected in a timely manner.
References/Bibliography: 1. IAEA Information For Health Professionals: Interventional Cardiology: http://rpop.iaea.org/RPOP/RPoP/Content/InformationFor/HealthProfessionals/ 5_InterventionalCardiology/phaseserythema.htm Accessed November 24, 2009. 2. FA Henry et al. Fluoroscopy-induced chronic radiation dermatitis: A report of three cases Dermatology online Journal, Vol 15, Number 1, January 2009. 3. AAPM Report No. 96, The Measurement, Reporting, and Management of Radiation Dose in CT. Report of AAPM Task Group 23: CT Dosimetry. Available at http://aapm.org/pubs/reports/. Accessed November 13, 2009. 4. Bauhs JA, Vrieze TJ, Primak AN, Bruesewitz MR, McCollough CH. CT Dosimetry: Comparison of Measurement Techniques and Devices. Radiographics 2008; 28:245-253. 5. ImPACT CT Patient Dosimetry Calculator, version 1.0 28/08/2009, http://impactscan.org Accessed November 13, 2009.