Download
1 / 16
160 likes | 331 Views
External Peer (Case) Review Peer Review Committee May 2012. Welcome. You are helping colleagues in other Oregon CAHS by providing true peer case review. Many of you have been doing case reviews already and your time is valuable so we will try to respect that today.

E N D
External Peer (Case) Review Peer Review Committee May 2012
Welcome • You are helping colleagues in other Oregon CAHS by providing true peer case review • Many of you have been doing case reviews already and your time is valuable so we will try to respect that today. • There may be portions of case reviews about which you are uncertain and we hope to make you feel more comfortable with doing these reviews.
Agenda • The Need for Case Review. • The People & Organizations Involved in the ORHQN Case Reviews. • Key Legal & Regulatory Information. • How to Approach Reviewing a Record. • How to Use the ORHQN Review Tools.
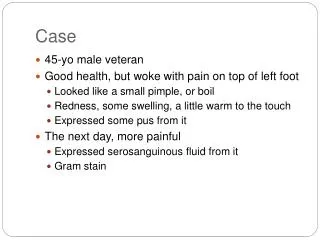
The Need for Case Review The principle reason for doing the case reviews To provide our fellow medical staffs with an independent look at the reasonableness of providers‘ documented actions during a patient's hospitalization. Hopefully the reviewer can identify opportunities for improvement. Example: trauma case Other reasons include: requirement for participation as a CAH, medical staff credentialing requirements. The point is that by doing them we all contribute our professional skills towards providing and improving care to patients served by CAHs in Oregon.
Who and What The Providers Involved in the Hospitalization The Peer Review Body of the Treating CAH Key Contact Person there to Coordinate Requests ORH (EJ) to Match Requests with Reviewers Key Contact at Reviewing Institution Receives and Distributes Request Reviewer (you) Completes the Review and Returns to your Key Contact Reverse the Flow Back to the Requesting Hospital ORHQN Provides the Oversight, Training, Finances and Evaluation
Review Request Flow Hospital Sending Hospital contact completes new row on Documents Sent Tracking form Hospital contact fills out request Hospital contacts ORHQN Coordinator for invoice and case number Hospital contact copies medical record, tabs sections & attaches form Hospital contact double wraps documents, stamps “Privileged and Confidential” and sends to ORHQN Confidential
Received Review Request Flow Receiving Hospital Hospital contact completes new row on Documents Received Tracking form and forwards records to physician for review Physician completes External Case Review Report and returns records and report to Hospital contact (30 day time frame) Hospital contact completes remaining fields on form and double wraps documents, stamps “Privileged and Confidential” and sends to ORHQN Confidential
KeyLegal & Regulatory Information Protected by ORS 41.675as a Peer Review Body Has all the confidentiality requirementsof a medical record under EMTALA There is a confidentiality agreement for all reviewersand reviewing institutions to sign prior to doing a review.
How to ApproachReviewing a Record Use the submitted record to review the providers' actions based on the information they had available to them at the time of that decision or action. Consider: A. Completeness was there sufficient information upon which to act. B. Commissions: what was done C. Omissions: what wasn't done that could reasonably have been done at that time. D. Reasonableness: was it clinically appropriate even though it may not be what the reviewer would have chosen to do. E. Consistencies: are the observations and actions of the providers seem consistent with that of other clinical staff. F. Timeliness.
Key Point as a Reviewer Identify but don’t speculate on the causes for a problem or missed opportunity. You are essential to the identification but it is the local Peer Review Committee that is in the best position to determine the causes.
Documents You Use & See Review Request Routine Review Review for Cause




![External Website Hosting Business Case [Free Template]](https://cdn4.slideserve.com/7373913/slide1-dt.jpg)