Download
1 / 54
550 likes | 823 Views
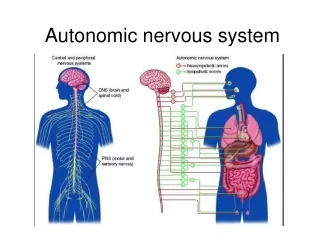
Autonomic Nervous System. Anatomical Division: Sympathetic (spinal cord: thoraco-lumbar) Parasympathetic (spinal cord: cranio-sacral) Functional Classification: Adrenergic Neurons ganglia - acetylcholine post-ganglionic neurotransmitter - norepinephrine Cholinergic Neurons

E N D
Autonomic Nervous System Anatomical Division: Sympathetic (spinal cord: thoraco-lumbar) Parasympathetic (spinal cord: cranio-sacral) Functional Classification: Adrenergic Neurons ganglia - acetylcholine post-ganglionic neurotransmitter - norepinephrine Cholinergic Neurons ganglia - acetylcholine post-ganglionic neurotransmitter – acetylcholine Nitrergic Neurons post-ganglionic neurotransmitter – NO
Fundamentals of Integrated Systems Outline for adrenergic & cholinergic pharmacology Overview: - anatomy of autonomic nervous system & transmitters - functional significance of sympathetic vs. parasympathetic - adrenergic vs. cholinergic synapse Adrenergic receptors: - subtypes (pharmacological evidence) - pharmacological effects of agonists & antagonists* Cholinergic receptors: - subtypes (pharmacological evidence) - effects of atropine* Nitrergic neurons, vasodilation, diabetes & Viagra®* Journal Club; Furchott & Zawadzki, Nature 288: 373, 1980* * test questions
key points • Significance of reflex • Rationale for specific pharmacological agonists & antagonists • note: potential for effect of an antagonist only if the susceptible system is activated • consider propanolol as an example
Significance of the Autonomic Nervous System Involuntary regulation - respiration - circulation - GI - GU - temperature - endocrine & exocrine glands Note: potential for dominance of voluntary control
Endocrine vs. Nervous Systems 40+ hormones a) tissue specificity based on chemical structure of hormone & receptor expression b) plasma t½ life reflects rate of hormone elimination c) feedback based on plasma hormone concentration d) presence/absence of stimulus or counter regulation 2 primary peripheral neurotransmitters (NE & ACh) – actually about 15 total (ex. NO) a) tissue specificity due to site-specific release b) local mechanisms for termination of transmitter action** -neuronal recapture via active transport (cocaine), then re-storage or metabolism (MAO inhibitors) -post-junctional metabolism (cholinesterase inhibitors) c) feedback based on synaptic transmitter concentration** c) reflex: feedback based on physiological effect** d) presence/absence of stimulus or counter regulation*** Drugs affecting the nervous system - analogous to hormones (no site specific release) - rationale for development of selective agonists & antagonists for pharmacological therapy
Sympathetic Nervous System Stress-induced activation: physiological responses to norepinephrine & epinephrine - conserve temperature - elevate blood glucose & FFA - redistribute blood to brain - accelerate heart rate & force of contraction - dilate skeletal muscle blood vessels - dilate bronchi & pupils - CNS activation (purposeful responses)
Parasympathetic Nervous System Regulation in a stress-free environment Physiological responses to post-ganglionic acetylcholine Inhibitory- hyperpolarize: slows heart Stimulatory- depolarize: stimulates digestive processes stimulates urination protects retina from excessive light (constriction of pupil)
note: dual innervation; parasympathetic at rest; sympathetic with stress
adrenergic vs. cholinergic dominance of major organ systems at rest
Sympathetic/Adrenergic Nervous System & Cardiovascular System: agonists & relevant receptors: NE for α1 (vasculature) & β1 (heart) Epi for α1 (most vasculature) & β1 (heart) & β2(bronchioles, skeletal muscle vasculature*, muscle tremor, glycogenolysis) Isoproterenol for β1 & β2 *skeletal muscle vasculature also expresses α1, but effects of β2 predominate
↑ heart (β1): Epi=NE=Iso ↓ sk mus arteriole (β2): Epi=Iso>>NE ↑ vasoconstriction (α1): Epi~NE>>>Iso NE for α1 & β1 Iso for β1 & β2 Note: - equal direct effects of NE, Epi & Isoon heart -recognize that pulse rate for NE would = Epi & Iso in presence of atropine
-agonists & therapy of asthma(rationale for selective agonists) Side Effects heart blood pressure glycogenolysis tremor* (direct/reflex) (heart/resistance) Epi (1 & 1 & 2)) Isoproterenol (1 & 2)) Terbutaline (2) * tolerance develops
Epinephrine & Allergic Reactions(itching, swelling, difficulty breathing, fainting) i) vasoconstriction (1) & cardiac stimulation (1) =↑ CNS perfusion ii) bronchiolar dilation (2) & reduced bronchiolar secretions (1) = improved ventilation iii) reduced histamine release (2) = ↓ itching & vascular permeability (swelling/edema) note: advantage vs. norepinephrine
propanolol Therapeutic uses: - hypertension- cardiac output & renin release (little effect in normotensive) - symptomatic panic- heart rate & tremor Side effects: - CNS (sedation, insomnia, nightmares) - decreased exercise tolerance - contraindication in asthma i) ii) - metabolic consequence in Type 1 diabetes i)
-adrenoceptors 2- adrenoceptor pre-junctional/pre-synaptic/nerve terminal 1- adrenoceptor: post-junctional/post-synaptic
1-adrenoceptor agonists Phenylephrine mechanism: selective α1-agonist use: nasal decongestant (inhalant) toxicity: hypertension in predisposed urinary retention in BPH
Selective 1-adrenoceptor antagonist phentolamine (non-selective antagonist) vs. prazosin (selective α1): Understanding the rationale for selective α1: - neuronal release - NE effect - net response
non-selective vs. selective α1-antagonists NE release post-junctional antagonism response (@ receptor) (contraction) control phentolamine (non-selective) prazosin (selective)
-adrenoceptor antagonists phentolamine (non-selective antagonist)vs. prazosin (selective α1): significance of selective post-junctional antagonism i) therapeutic effect (hypertension & BPH) ii) side effect of selective α1 a) (think perfusion) b) (think reflex) c) rationale for bed-time administration
Indirectly & Mixed Acting Sympathomimetics & Toxicitypredictable & unpredictable side effects Amphetamine orally active indirect acting Ephedrine mixed (indirect + & ) Cocaine blocks neuronal uptake of released NE “Fen-Phen” fenfluramine-phentermine (serotonin agonist-amphetamine like analog) fibrosis of heart valves - $$$
monoamine oxidase inhibitors:mechanism of action & the “cheese effect” • Mechanism of action • Rapid and irreversible inhibition of MAO-A in a few days • Increased intra-neuronal NE reduces gradient for neuronal re-uptake of released NE • Increased synaptic concentrations of NE • However, clinical effect as anti-depressant requires few weeks • Due to adaptations in CNS receptors ? (Murphy in Psychopharmacology 1987) • Cheese effect • Inhibit intestinal MAO-A with oral administration • Ingest foods with tyramine (cheese, red wine) • tyramine is not inactivated (not deaminated by MAO-A) & absorbed • Indirectly acting sympathomimetic • Consequence?
Peripheral Cholinergic (Ach) Receptors Muscarinic receptors: (blocked by atropine) post-ganglionic sites: cardiac & smooth muscle & epithelium of glands Nicotinic receptors: autonomic ganglia (blocked by hexamethonium) skeletal muscle endplate (blocked by tobocurarine)
Cholinergic Receptor Sub-types Muscaranic: - 5 sub-types - G-protein coupled to activate phospholipase C (smooth muscle contraction & glandular secretion) or inhibit adenylate cyclase (heart) Nicotinic: - as many as 11 sub-types - ligand-activated ion channels increasing sodium & calcium permeability
Endogenous cholinergic transmitter at all sites Cholinergic antagonist at ganglia Cholinergic agonist for ganglia & skeletal muscle Cholinergic antagonist at skeletal muscle) nicotinic receptor pharmacology
focus: muscarinic receptor pharmacology Cholinergic agonist at post-ganglionic sites other than skeletal muscle) Selective muscaranic antagonist
Understanding the effects of atropine (muscaranic antaginist)
Therapeutic uses of muscarinic antagonists GI ulcers opthalmology excessive respiratory secretions (anesthesia) excessive bradycardia (acute MI) Parkinson’s disease motion sickness **bladder instability (enuresis; urge incontinence)
Common Side Effects of a muscarinic antagonist when used for incontinence 1) 2) 3) 4) 5)
experimental information & questions for test Atropine: - no effect on blood pressure at rest ACh: - vasodilation - competition by atropine why was atropine ineffective when given alone? response to very high doses of Ach + atropine = ?
experimental design:i.v. drug administration in anesthetized dog - record mean blood pressureexperimental findings:
Test Question: In Vivo experimental demonstration of: 1) absence of significant cholinergic innervation to the arterioles (resistance vessels) 2) presence of functional cholinergic (muscarinic) receptors in resistance blood vessels 3) competitive antagonism by atropine 4) mechanism of vasodilation 5) ACh-induced ganglionic transmission & Epi release
Experimental analysis of the effect of Ach ± atropine on B.P.
Mechanism of ACh-induced vasodilation - indirect effect via endothelium - ACh via muscaranic receptor on endothelial cells - increased endothelial NO synthesis from arginine - NO-induced smooth muscle relaxation - cyclic GMP protein kinase Ca++ & Ca++ sensitivity of cross bridge formation (Ann Med 35:21,2003 & J Cell Physiol 184:409,2002)
Rationale for sildenafil (Viagra®) use in erectile dysfunction of diabetes? neurological? vascular?
Cholinergic Neurotransmission:Release Acetylcholine release - action potential-induced quantal release (all or none) of vesicles - inhibited by botulinum toxin (motor neuron) (proteolysis of proteins necessary for ACh quantal release) - inhibited by tetanus toxin (spinal cord neuron) (retrograde migration through nerve to spinal cord to block transmitter release from inhibitory neurons- spastic paraylsis of skeletal muscles “lock jaw”
adrenergic vs cholinergic synapse differ qualitatively with respect to termination of neurotransmitter action
Uses & Toxicity of Cholinesterase Inhibitors Uses: Glaucoma Myasthenia gravis **Insecticide (low human/bird toxicity due to rapid inactivation) Chemical warfare compounds Toxicity: muscarinic (visual, respiratory, S.L.U.D.) nicotinic (respiratory paralysis)