Download
1 / 15
160 likes | 340 Views
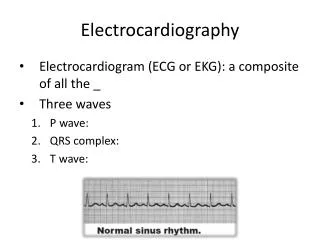
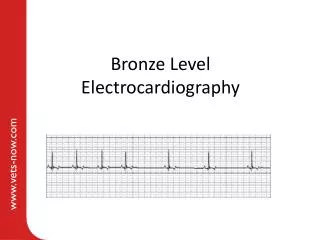
Bronze Level Electrocardiography. Aims. Brief summary of relevant clinical electrophysiology Indications for taking an electrocardiogram (ECG) How to obtain a diagnostic ECG All Covered in Part 1 Basic ECG interpretation. Section 4 – basic ECG interpretation.

E N D
Aims • Brief summary of relevant clinical electrophysiology • Indications for taking an electrocardiogram (ECG) • How to obtain a diagnostic ECG All Covered in Part 1 • Basic ECG interpretation
Premature QRS complexes – wide or narrow QRS morphology Trace 1 Both of these traces show premature QRS complexes. These are complexes with a shorter R-R interval than the preceding sinus beats Trace 2
Trace 1 Trace 1: The first 4 complexes show sinus rhythm. The 5thQRS complex is a premature beat with no associated P wave and a wide bizarre QRS morphology which suggests that it is not being conducted through the ventricles via the normal conduction system. As this beat originates in the ventricles it is termed a ventricular premature beat or VPC. The remainder of the trace shows sinus rhythm.
Trace 2 Trace 2: Shows premature narrow QRS complex beats (the 2nd, 5th, 8th, 11th and 14th beats). These are supraventricular premature beats or SPC.
Escape beats Sinus arrest with ventricular escape rhythm Sinus rhythm Escape beats are less common than premature beats Escape beats occur after an interval GREATER than the normal R-R interval (cf premature beats occur after an interval LESS than the normal R-R interval) Escape beats have a wide and bizarre complex morphology as they originate from the ventricles. Escape beats maintain cardiac output during sinus arrest.
Potentially life threatening ECGs – ventricular tachycardia Sinus rhythm Ventricular tachycardia • Characteristics of VT: • Rapid (>180bpm) • Generally regular • More than 6 consecutive wide, bizarre QRS complexes • Seen in animals with severe cardiac and/or systemic disease (eg gastric dilation torsion, pancreatitis, splenic disease, IMHA, etc). • Of particular concern in Boxers, Dobermanns and Great Danes
Potentially life threatening ECGs – coarse ventricular fibrillation Ventricular fibrillation is characterised by very rapid baseline undulations.
Potentially life threatening ECGs – fine ventricular fibrillation Usually a terminal rhythm Rapid baseline undulations of lower amplitude to coarse VT. In this cases progresses to complete asystole and death around 11:27.
Potentially life threatening ECGs - asystole Flatline as there is no organised atrial or ventricular activity
Potentially life threatening ECGs – high grade second degree atrioventricular block P P P P P P P P P QRS T Large number of consecutive unconducted P waves (blocked at atrioventricular node or AVN). Finally a P wave is conducted through the AVN resulting in a normal QRS complex. There are then 13 consecutive unconducted P waves before the next P-QRS-T complex.
Potentially life threatening ECGs – sinus arrest with very slow escape rhythm During this 10 second period only a single beat is seen therefore the heart rate is very slow during this recording. The beat seen has a bizarre QRS morphology and is not preceded by a P wave suggesting that it is ventricular in origin.